Full chapter reading
Chapter 11: Tailored Fitness Assessments and Program Design for Special Populations
Introduction
This chapter provides additional guidelines and considerations to the initial consultation, along with guidelines and suggestions related to the design of cardiovascular, resistance training, flexibility, and trigger point, programs.
Like the initial consultation for an able-bodied individual without known chronic diseases or musculoskeletal issues, the first step for individuals in the "medical fitness" category is to complete the exercise pre-participation health screening and Physical Activity Readiness Questionnaire (PAR-Q) outlined in Chapter 3. However, the key distinction for those in the medical fitness category lies in the presence of one or more conditions, which influence the consultation, initial assessment, and exercise program design.
Step two involves a detailed discussion about their condition(s) and identifying any necessary program modifications.
If the client needs medical clearance, or acute care, they should be referred to the appropriate medical provider before engaging in a training program. If they do not require medical clearance or have already received it, and do not need acute care, the individual can engage in an appropriately designed exercise program as described in this book.
Section 1: Additional Consultation Considerations and Guidelines
Different scenarios in how the potential client was referred lead to slight differences in the approach for the initial medical fitness consultation. Overall, the general guidelines and considerations are very similar.
Three scenarios that will be covered in this section are:
- The fitness professional works within a clinical setting and the patient/potential client was referred via a medical professional.
- The fitness professional works outside of a clinical setting and the patient/potential client was referred via a medical professional.
- The fitness professional works outside of a clinical setting and the potential client was obtained by means other than through a medical professional (e.g., approached on the gym floor, referred through a family member, obtained via online advertisement, etc.).
Scenario 1: The fitness professional works within a clinical setting and the patient/potential client was referred by a medical professional.
If the fitness professional has direct access to the Electronic Medical Record (EMR) the first step is to access the EMR and begin to gather information about the patient prior to meeting them. This can include their height, weight, medications, and the notes entered into the system during past visits. This allows the fitness professional to gain valuable insight into why the patient was being seen, what their conditions are, and any specific recommendations the care team has for the patient.
If the fitness professional works in a clinical setting but does not have direct access to the EMR, they have two options:
Option 1: Approach the medical professional who referred the patient immediately after the initial consultation to obtain insight and advice about the patient.
In this case, the fitness professional will learn about the potential client’s conditions, apprehensions, needs, and goals during the initial consultation. Armed with this information, the fitness professional then approaches the referral source and says:
“Thank you for the referral. I met with your patient for the initial consultation, and we reviewed their issues/conditions, needs, and goals. Before I design an exercise program, please let me know what you would like me to emphasize within their program (indications), what you would like me to avoid (contraindications), and if there is anything else you would like me to know about this patient (e.g., psychosocial issues, financial issues, travel issues, etc.).”
If the patient was referred by a physical therapist, the fitness professional should gather key information from the therapist, including the therapeutic exercises the patient started with, their progress to date, and any specific recommendations for the fitness professional to emphasize or avoid. Additionally, they should seek any other relevant details that could inform the patient's exercise program.
Option 2: Approach the medical professional who referred the patient prior to the initial consultation. Thank them for the referral and ask the same general questions. In this case, the fitness professional is armed with less information since they have yet to meet with the potential client.
It is critical to connect with the referral source either before or after the initial consultation to obtain information and bridge the gap.
Scenario 2: The fitness professional works outside of a clinical setting and the patient/potential client was referred by a medical professional.
In this instance, the fitness professional will not have access to the EMR but does have direct access to the referral source. The same concepts apply as stated above with one difference:
Since the fitness professional doesn’t work directly with the referral source, they should contact them immediately before or immediately after the initial consultation to find out what the referral source would like to see emphasized, avoided, and any other pertinent information they would like to convey.
Scenario 3: The fitness professional works outside of a clinical setting and the potential client was obtained by means other than through a medical professional (e.g., approached on the gym floor, referred through a family member, obtained via online advertisement, etc.).
In this situation, the fitness professional will not have access to the EMR and does not have direct access to the referral source. The fitness professional should conduct the initial consultation with the potential client, during which time they can obtain approval from the client to contact the appropriate medical professional (e.g., family physician, cardiologist, physical therapist, etc.).
In most cases, the client will give their approval. The fitness professional can then obtain the medical professional’s contact information (e.g., email address) or stop by their office to speak with a front desk administrator. In the latter case, the fitness professional can explain to the administrator that one of their clients is a patient of the medical professional and ask what the best way is to contact them is to ask relevant questions prior to designing an exercise program.
If the client is not able or willing to provide their medical professional’s contact number, the fitness professional must decide if they feel it is appropriate to train this client. The fitness professional can take a detailed history and request that the client bring a summary of their health issues from their providers office to confirm what the patient said.
Bridging the medical-fitness gap requires establishing a strong connection with the medical professional, making it essential for the fitness professional to prioritize this collaboration and proactively gather the necessary information.
Accessing Additional Information
If a potential client presents with a disease or metabolic condition beyond the fitness professional's expertise and is not addressed in this book, it's advisable to conduct further research post-consultation. The Centers for Disease Control and Prevention (CDC) offers general information on various diseases and conditions at https://www.cdc.gov/diseasesconditions/index.html. Additionally, the National Library of Medicine's PubMed database (https://pubmed.ncbi.nlm.nih.gov/) provides access to primary literature on specific diseases, conditions, and treatments. Consulting the official website of the relevant disease or condition's governing body can also yield valuable insights.
During the initial consultation, the fitness professional will need to obtain information in addition to the client’s perceived needs, goals, and exercise/training history as mentioned in Chapter 3. This will include the need to discuss all pertinent information about the client’s disease and musculoskeletal history, medications, and how the medications may affect exercise. The fitness professional should ask the client the following questions:
- How does your condition(s) affect your activities of daily living and while you exercise?
- How did your condition(s) begin? Tell me about the progression. How are things now? Have you improved? What led to the improvement (or worsening)?
The answers to these important questions will give insight into the client’s condition(s), concerns, mindset, apprehensions, and restrictions or limitations. This will be critical information to consider when designing the program.
Silent Diseases
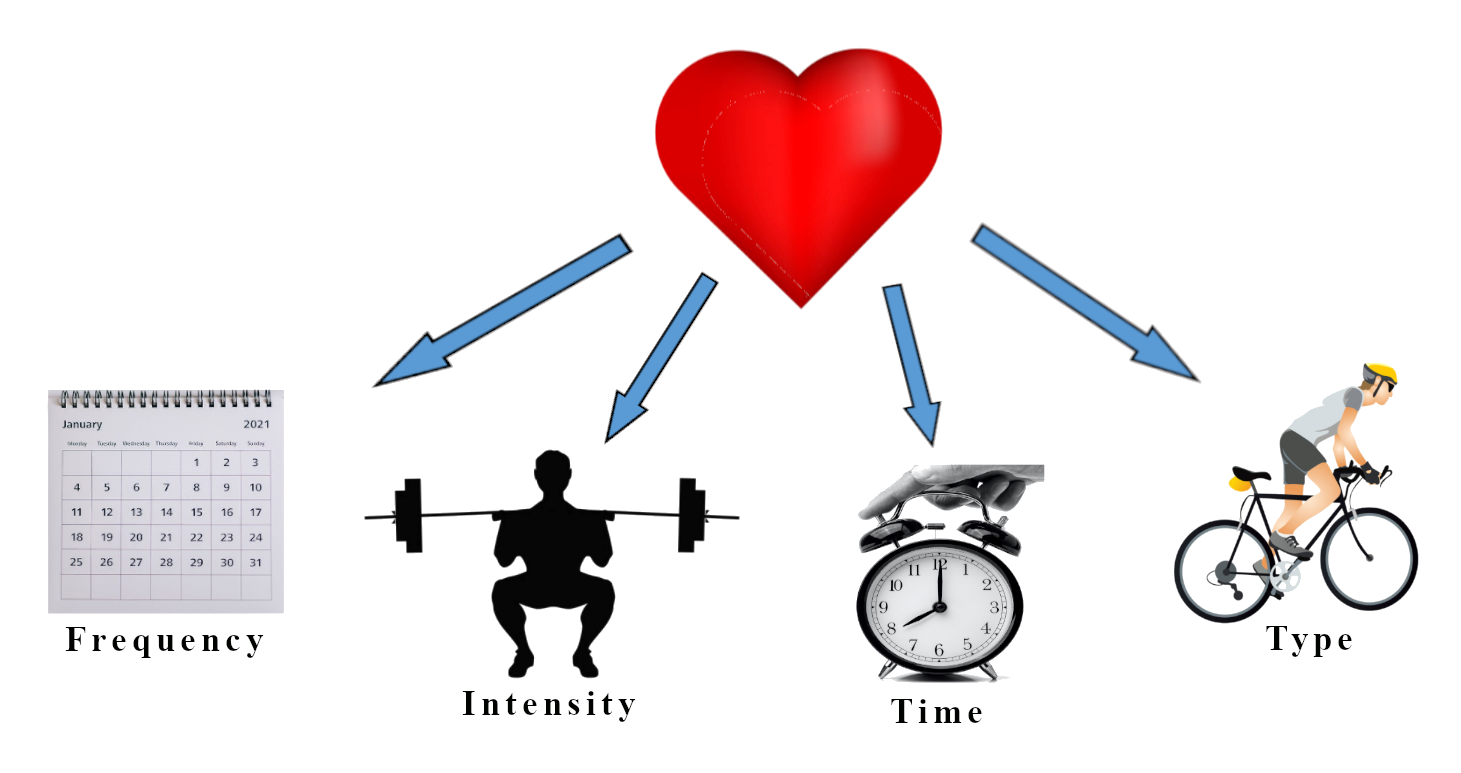
Some conditions don’t manifest themselves in the form of pain, discomfort (i.e., a flare-up or exacerbation), or obvious symptoms, such as hypertension. For conditions that do manifest themselves in the form of an acute exacerbation the fitness professional can use the general concept behind the F.I.T.T. Principle to gain additional insight into the condition(s) by asking:
- What is the frequency of your flare-up(s)?
- When you have a flare-up, what is the intensity and type (e.g., sharp, stabbing pain; headaches, nausea).
- When you have a flare-up, how long does it typically last (time)?
Figure 11.1: F.I.T.T. Principle
There may be occasions where the fitness professional will realize that the patient’s condition is not stable enough or appropriate for training and, as previously mentioned, may need to refer the client out to a healthcare professional.
Summary
In summary, this section outlines the process for medical fitness consultations, emphasizing the importance of tailoring exercise programs to individuals with chronic conditions or musculoskeletal issues. The process begins with a health screening, the PAR-Q, and a discussion about the client’s condition(s) to identify necessary program modifications. Clients requiring medical clearance or acute care must be referred to a healthcare provider before starting.
The section addresses three scenarios:
- Within a Clinical Setting (Medical Referral): Use the EMR or consult the referring provider for relevant information.
- Outside a Clinical Setting (Medical Referral): Contact the referral source to obtain guidance before or after meeting the client.
- Self-Referred or Non-Medical Referral: Seek client permission to consult their healthcare provider or proceed cautiously based on the available information.
Fitness professionals should gather detailed insights into the client’s condition(s) and assess symptomatic issues using tools like the F.I.T.T. Principle. For conditions beyond the fitness professional’s expertise, reputable resources such as the CDC or PubMed can provide further guidance. If the client’s condition is unstable, a referral back to a medical professional is required, ensuring safety and bridging the medical-fitness gap effectively.
Section 2: Additional Strength Assessment Considerations and Guidelines
Unlike the guidelines provided in Chapter 6 for an able-bodied exerciser, where the fitness professional or individual may choose between maximal strength testing (e.g., 1 to 6RM bench press) or The RPE Method approach, special populations should not undergo maximal strength testing. It is often impractical and frequently unsafe to perform maximal or near-maximal initial testing with special populations. Instead, the fitness professional or individual should rely solely on The RPE Method.
Initial loads should be conservative (e.g., corresponding with an RPE of 5 on a 1 to 10 scale) and chosen during the Familiarization Phase based on The RPE Method. This same method should be used to guide safe progression as well.
Refer to Chapters 3, 4, and 6 (and the corresponding videos found at www.MRFInstitute.org) for more information on how to use The RPE Method to determine initial loads and incorporate these concepts to guide safe progression.
Section 3: Additional Trigger Point Release Assessment and Program Design Considerations and Guidelines
Fitness professionals or individuals should perform a trigger point release assessment to determine where trigger points exist to individualize the program.
The assessment may need to be adjusted for individuals who have difficulty getting down to or up from the floor. Modifications can include evaluating trigger points while the individual is seated or using supportive props placed between them and a wall to provide stability and accessibility.
Refer to Chapter 7 for images of trigger point release using tools, or props, against the wall, or the corresponding video (www.MRFInstitute.org) for even more detailed information. Below are images using “The Stick” while seated. Any tool that adequately presses into soft tissue can be used to “seek out” trigger points. The person does not need to go to the additional expense of purchasing expensive tools. “The Stick” is used in the images, but a simple dough roller found in many homes is sufficient.
Figure 11.2: Trigger Point Release Using “The Stick.”
Figure 11.2: Trigger Point Release Using “The Stick.”
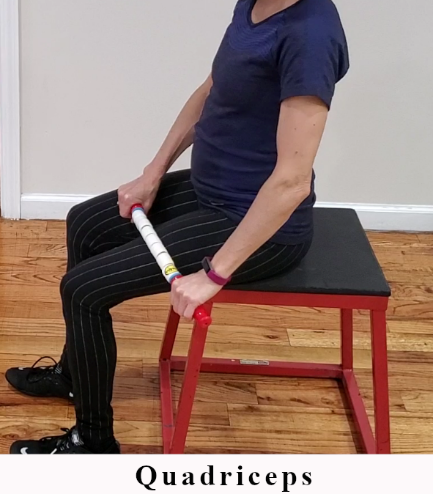
Quadriceps

IT Band

Hamstrings
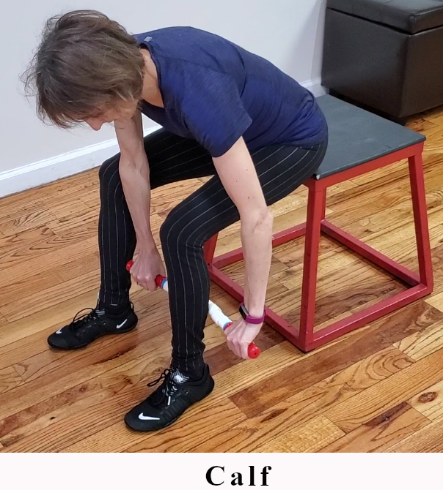
Calf

Peroneals
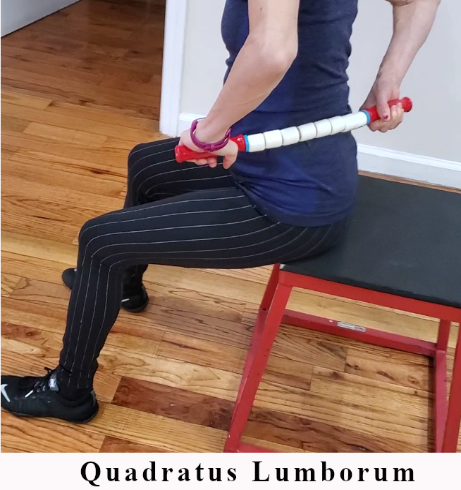
Quadratus Lumborum
Section 4: Additional Flexibility Assessment and Program Design Considerations and Guidelines
Prior to training any population – special, general, or athletic – ideally, a joint range of motion assessment should be performed. This information should be used to place the individual on a proper flexibility program designed to balance flexibility around each major joint and remove movement restrictions (areas of tightness).
Information gathered from the referral source (if applicable) on possible sites of injury and stages of healing, along with the information gathered from the client themselves during the initial consultation may reveal an area (or areas) of the body that will need to be avoided during the initial joint range of motion assessment. This is particularly applicable to people with musculoskeletal conditions. Care must be taken with these individuals to preclude assessing any joints or areas of the body that may be problematic.
When performing the assessment, the fitness professional should move joints slowly through their range of motion, stop the movement shy of the end range of motion, if applicable, and pay special attention to their feedback – both verbal and visual (e.g., a look of apprehension or discomfort).
Designing flexibility programs for special populations otherwise adhere to what was described in Chapter 7 and the corresponding video found on the MRF Institute website. Avoid stretching all areas where there exists pain or discomfort. When stretching, individuals should only feel the sensation of a light to moderate stretch.
Section 5: Additional Cardiovascular Assessment Considerations and Guidelines
The cardiovascular assessment and program design guidelines for special populations are identical to the suggestions noted in Chapter 5, Section 2. Additional considerations for special populations include:
Ensure that the individual displays no signs or symptoms with respect to cardiovascular (CV), metabolic (i.e., diabetes), or renal (kidney) disease at rest or during exercise (Table 11.1):
Table 11.1: Signs and Symptoms Indicative of Severe Disease
Table 11.1: Signs and Symptoms Indicative of Severe Disease
| Sign or Symptom | Description |
|---|---|
| Pain or discomfort | Pain in the chest, neck, jaw, arms, or other areas. |
| Shortness of breath | Difficulty breathing at rest or with mild exertion. |
| Dizziness or syncope | Temporary loss of consciousness or feeling lightheaded. |
| Orthopnea or paroxysmal nocturnal dyspnea | Shortness of breath when lying supine or severe nighttime shortness of breath and coughing. |
| Ankle edema | Swelling in the ankles, potentially indicative of congestive heart failure or a vein blockage in the leg. |
| Palpitations or tachycardia | Fast resting heart rate or a fluttering sensation in the chest. |
| Intermittent claudication | Aching or burning pain in the legs, typically caused by poor circulation. |
| Known heart murmur | Abnormal heart sounds that may indicate underlying cardiovascular issues. |
| Unusual fatigue or shortness of breath | Fatigue or difficulty breathing during normal, everyday activities. |
- Obtain medical clearance when appropriate (refer to Chapter 3 for more information).
- Start low and progress slow.
- Obtain regular feedback from the individual when performing the initial assessment and during cardiovascular exercise within training sessions.
- Use the RPE scale and Talk Test (RPE-Talk Test) as the primary guides to determine exercise intensity.
- Ensure the exerciser has established a baseline level of fitness – the ability to sustain a minimum of 15 to 20 minutes of continuous aerobic exercise at 70% of maximum heart rate or above (i.e. the middle of the heart rate training zone; an RPE of 5 to 6) – before progressing to high intensity interval training or modified high intensity interval training (e.g. interval walking program) (Ribeiro, 2017).
- Take any musculoskeletal or balance issues into consideration when determining mode of exercise. For example, a person with balance issues should not be asked to perform the treadmill exercise. A person with knee or hip issues may need to be advised to swim or perform aerobic exercise on the elliptical machine, depending on the severity of symptoms.