Full chapter reading
Chapter 12: Musculoskeletal Conditions and Osteoporosis
Introduction
The human musculoskeletal system and skeletal health are pivotal to maintaining mobility, reducing injury risk, and supporting overall physical function. This chapter is divided into two primary sections, addressing common musculoskeletal (MSK) conditions and osteoporosis. Each section provides a comprehensive framework for understanding and designing effective exercise programs tailored to these specific concerns.
The first section focuses on MSK conditions, emphasizing the importance of addressing key components such as neuromuscular control, strength, joint stability, and mobility. It outlines strategies for working around pain or injury, restoring functional movement, and promoting long-term musculoskeletal health through progressive strength and conditioning.
The second section centers on osteoporosis, a condition characterized by weakened bones and increased fracture risk. Here, the chapter provides evidence-based guidelines for safe and effective exercise interventions that improve bone density, muscular strength, and balance. It also highlights the importance of avoiding movements that may exacerbate bone fragility while promoting functional independence and injury prevention.
Through these sections, this chapter equips fitness professionals and individuals with practical tools to optimize skeletal and joint health, manage pain, and enhance quality of life across diverse populations.
Section 1: Program Design Considerations and Guidelines for Common Musculoskeletal Conditions
While diagnosing or treating injuries falls outside the scope of a fitness professional’s practice, they still play a crucial role in addressing musculoskeletal (MSK) conditions by designing safe and effective exercise programs. These programs can prevent, manage, or even improve MSK conditions by working around pain or injury, restoring strength, mobility, and stability, and promoting overall conditioning. This approach applies to both fitness professionals and individuals exercising independently and includes:
- Avoiding painful areas when necessary.
- Adjusting foot, hand, or joint positions to alleviate discomfort.
- Modifying range of motion or load to ensure pain-free movement (Kompf, 2014).
At its core, this chapter provides a universal approach to MSK program design, emphasizing that regardless of the specific condition or location, the foundation of a healthy musculoskeletal system depends on addressing six primary components:
- Neuromuscular Control (NMC): The ability of muscles to work together efficiently, ensuring proper form and movement patterns.
- Strength: The maximum force a muscle group can produce. Increasing strength improves the capacity to tolerate loads and stressors, reducing the risk of injury.
- Strength-Endurance (Stamina): The capacity to maintain strength under fatigue, critical for preventing injuries.
- Joint Stability: The ability of muscles and connective tissues to stabilize joints during movement.
- Posture and Alignment: Balanced strength and mobility to maintain proper joint positioning.
- Mobility: The intersection of flexibility and strength, ensuring usable range of motion in dynamic, loaded conditions.
By addressing these components through progressive strength and conditioning programs, fitness professionals and individuals can create a comprehensive plan to reduce pain, improve movement efficiency, and promote long-term musculoskeletal health.
Integrity of a Joint
Joint health is maintained by both structural and functional components. Structural elements, such as joint congruency (alignment of joint surfaces) and soft tissue integrity (e.g., ligaments, tendons, cartilage), provide stability, transfer force, and facilitate efficient movement. However, when these structures are compromised by injury, inflammation, or degeneration, the musculoskeletal system relies heavily on muscle strength to compensate.
Strong, conditioned muscles absorb and distribute forces, reducing stress on joints and soft tissues. This makes strength development a cornerstone of managing MSK conditions. A properly designed program that strengthens both global and intrinsic muscles around each joint is key to improving joint function, stability, and resilience. This foundational concept is expanded upon throughout the chapter, with practical strategies for addressing specific conditions like knee, back, shoulder, and neck pain.
Mechanisms Associated with Injury or Pain
Various factors contribute to increased risk of injury or pain, including:
- Improper form under heavy loads or fatigue, underscoring the importance of neuromuscular control and proper technique.
- Insufficient warm-up, especially before high-intensity or explosive movements.
- Repetitive stress, leading to microtrauma and chronic inflammation.
- Movement restrictions (tightness), impairing joint mobility.
- Lack of stability under load, particularly when tissues are stressed at end-range positions or under unfamiliar loads.
The Cause of Injury

Despite these contributing factors, all injuries share a common cause: tissue failure under stress. In the moment of injury, the affected tissue lacks the capacity to tolerate the force applied (e.g., shear, compressive, or torque forces).
To mitigate this, programs should focus on gradually improving the tissue's ability to tolerate stress, increasing both strength and conditioning, while addressing mobility and stability deficits. This is achieved through progressive strength and conditioning programs tailored to the individual’s specific condition.
Universal Principles of MSK Program Design
A universal approach applies to all MSK conditions, focusing on:
- Improving mobility where restrictions exist.
- Increasing strength where weakness or hypermobility is present.
- Progressing individuals out of the beginner strength domain by using the strength domains as points of reference and goals to achieve (Figure 12.1, Chapter 6).
- Ensuring proper form to reinforce neuromuscular control and prevent compensatory patterns.
Figure 12.1: Fitness Level Continuum
Fitness Level Continuum
A polished continuum showing the same source progression from Beginner through Elite.
This approach naturally improves the six components of a healthy musculoskeletal system, promoting better movement efficiency, reducing pain, and increasing the body’s resilience to injury.
Why Most Individuals Need This Approach
Approximately 80% of adults fail to meet the minimal strength training guidelines (CDC, 2008–2017). As a result, many individuals are weak, deconditioned, and have imbalances that increase their risk for MSK injuries. By simply adhering to a properly designed, progressive strength and conditioning program, most individuals can achieve significant improvements in strength, mobility, and stability. Programs should:
- Use pain-free ranges of motion.
- Consider specific precautions for conditions (e.g., avoiding excessive lumbar extension for stenosis or deep knee flexion for severe osteoarthritis).
This method not only manages MSK conditions but often helps to heal them by strengthening and balancing the entire body.
Parallels with Physical Therapy
Figure 12.2: Physical Therapy Progression Stages
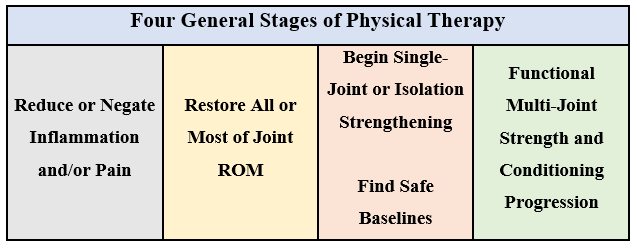
The four general stages of physical therapy align closely with the principles of progressive strength and conditioning:
- Reduce swelling and pain, allowing tissue healing.
- Restore joint mobility, ensuring pain-free movement.
- Establish safe baselines for load, volume, and exercise selection, often with a focus on single-joint movements and balance training.
- Progress loading and complexity, incorporating multi-joint, kinetic chain exercises.
In physical therapy, as pain subsides and mobility is restored, the focus shifts toward strength and conditioning to build resilience and prevent future injuries. Fitness professionals play a critical role in continuing this progression, bridging the gap between therapy and long-term physical fitness. A cohesive medical team, where each professional contributes their expertise, ensures the individual’s health and well-being.
Summary
For every orthopedic condition, the following principles form the foundation of effective exercise program design:
- Release trigger points and address movement restrictions (Chapter 7).
- Improve flexibility and joint mobility where needed (Chapter 7).
- Progressively strengthen and condition the entire body, ensuring balanced strength around each joint (Chapters 4-6).
- Prioritize proper form, as it reinforces neuromuscular control and prevents compensatory patterns (exercise technique videos found at www.MRFInstitute.org).
This holistic approach addresses the six components of musculoskeletal health, creating a universal framework for preventing, managing, and healing MSK conditions. By following these principles, individuals can achieve greater movement efficiency, reduced pain, and enhanced overall physical function.
The following sections provide general guidelines and considerations for individuals who present with knee, low back, shoulder, and neck pain.
The Knee
Knee pain is one of the most common conditions that individuals suffer from and comes in many forms, including but not limited to: chondromalacia, patellofemoral syndrome, and osteoarthritis (Bunt, 2018). For most non-acute situations involving a knee injury or pain, the modifications suggested below can be useful.
There are seven primary lower body movements/exercises:
- Squat variations
- Deadlift variations
- Lunge variations
- Hip thrust variations
- Leg press variations
- Step-up variations
- Horizontal push and pull variations (sled push and pull)
Most stress on the knee occurs within the first 60 degrees of flexion (Schoenfeld, 2010). After 60 degrees of flexion stress begins to shift to the hips, which is optimal. If the person is unable to reach a squat depth whereby knee flexion has reached at least 60 degrees, the fitness professional should discard squats from the program design, at least initially.
Figure 12.3: Quarter, Half, and Full Squat Examples.
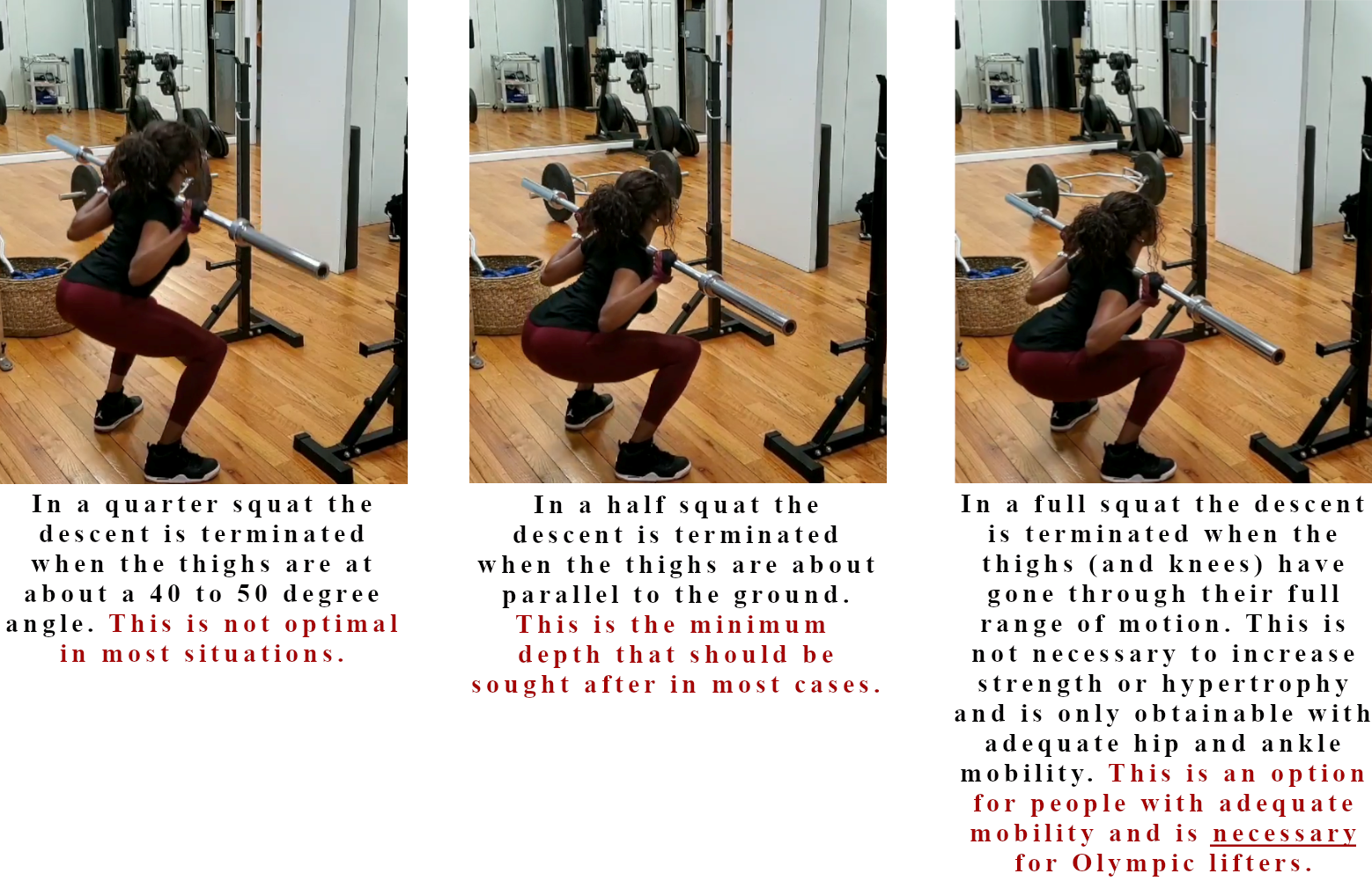
If it is contraindicated, or the person is unable to perform a squat at the appropriate depth, this exercise can be substituted with another lower body strengthening exercise. The following lower body strengthening exercises are considered “knee-friendly”:
- Hip thrusts
This is because there is little knee flexion and the emphasis is on the hamstrings and glutes, which create stability at the knee when contracting against proper loads.
- Deadlift variations
This is also because there is little knee flexion and the emphasis is on the hamstrings and glutes, which create stability at the knee when contracting against proper loads.
- Leg press
Range of motion may need to be shortened to determine the pain-free range of motion the exerciser can work within, starting very conservatively with the load selection and initial range of motion. As with all multi-joint, lower body exercises, the person must be instructed to ensure weight distribution at the foot is always towards the mid-to-hindfoot. This helps reduce stress at the knee and emphasize the musculature that stabilizes the knee.
- Knee curl exercises
These are hamstring strengthening exercises which assist in stabilizing the knee.
- Knee extension exercises within pain-free joint range of motion
When appropriate loading and joint range of motion are selected, this quadriceps strengthening exercise helps with knee stabilization and overall resiliency of the knee joint tissue.
- Calf raise exercises with the knee extended (i.e. a straight leg)
The gastrocnemius crosses the knee and acts as a knee stabilizer, along with assisting in force reduction. Strong calf muscles optimally stabilize and reduce force at the knee.
- Gluteus medius strengthening exercises
The gluteus medius assists in preventing and managing knee pain by reducing dynamic knee valgus (i.e., “caving in” at the knee) forces.
- Core strengthening exercises
Strengthening the core assists in stabilizing the pelvis, which helps stabilize the lower body kinetic chain.
- Squat and lunge variations
Depending on the knee condition and the severity of the condition, squat and lunge variations may be knee friendly. Examples include goblet squats, front squats, high-bar back squats, and backward lunges.
It is the fitness professional or exerciser’s responsibility to determine exercise selection, joint angle, pain-free range of motion, proper loading, and proper progression. Always avoid exercises that cause or exacerbate pain.
For additional clarity on knee-friendly concepts and exercises, view the related video found at www.MRFInstitute.org.
The Low Back
Low back pain is the fifth most common reason for all physician visits and is the second most common symptomatic reason that patients see a physician. In a medical fitness situation, (i.e., post-rehabilitation training or if no rehabilitation therapy was indicated), the following describes a safe approach for most conditions in most situations:
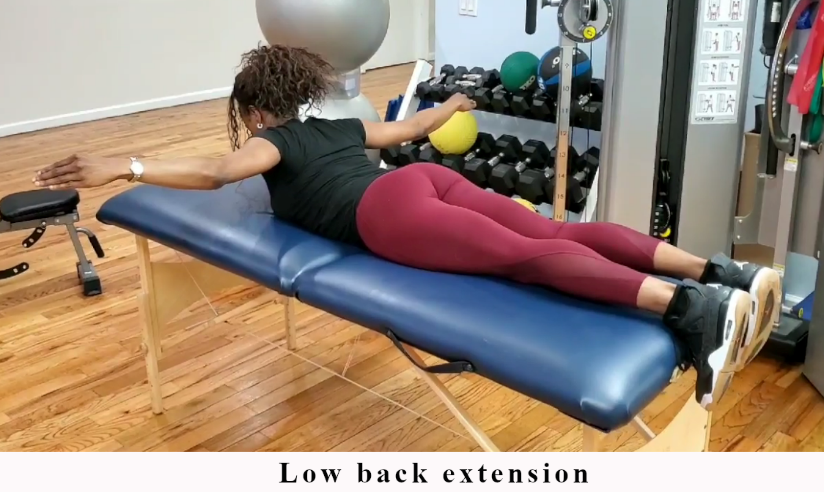
When the trunk muscles contract isometrically, maintaining spinal stability without movement, and exercises are performed with proper frequency, volume, duration, intensity, and form, the risk of injury or exacerbating existing conditions is significantly reduced. Therefore, before progressing to core strengthening exercises involving spinal flexion, extension, rotation, or lateral bending, fitness professionals and exercisers should prioritize movements that ensure trunk stability.
Figure 12.4: Core Strengthening Stabilization Exercises.
Figure 12.4: Core Strengthening Stabilization Exercises.

Example 1

Example 2

Example 3

Example 4

Example 5

Example 6
Example 7

Example 8

Example 9

Example 10

Example 11

Example 12
It is recommended that the individual begin by maintaining low frequency (e.g., two to three times per week), volume (one to two sets), and intensity (RPE = 4 to 6). Exercises can be programmed in two to four-week phases, during which time it should be ensured that the exerciser’s body is responding positively (e.g., no excessive soreness and the exercises are not causing or exacerbating joint pain).
The exerciser can then progress by increasing volume or intensity, or by introducing more challenging exercises over time.
Once it has been determined that a baseline level of strength and strength-endurance is obtained (e.g., a front plank can be held for at least 60 seconds, and a side plank can be held for at least 30 seconds), they can begin incorporating core exercises whereby the trunk is moving (i.e., “movers”). These include spine flexion (e.g., crunches), rotation (e.g., cable rotation), and lateral bending (e.g., oblique raises).
When “movers” are initially introduced into the program, the exerciser should greatly reduce joint range of motion. This reduced range of motion should be gradually increased in two to four-week phases. Individuals should avoid exercises that take the spine through full range of motion in flexion, rotation, lateral bending, and extension.
Excessive spine bending and loading in various directions (i.e., flexion, rotation, lateral bending, extension) may be contraindicated in conditions such as spinal stenosis, spondylosis, spondylitis, spondylolysis, spondylolisthesis, herniated disks, arthritis, and scoliosis. However, in non-acute situations the exerciser will be able to move and load the spine to some degree with any of these conditions. Safe starting points (limited range of motion), slow progression, avoidance of training to “at or near” end range of motion, and the use of light to moderate loads are safe in most situations. It is the fitness professional or exerciser’s responsibility to determine the safety and efficacy of exercise selection, proper loading (using The RPE Method), and optimal joint range of motion on a case-by-case basis (Table 12.1).
Table 12.1: Guidelines for Safe Spine Loading and Movement in Common Spinal Conditions
Table 12.1: Guidelines for Safe Spine Loading and Movement in Common Spinal Conditions
| Condition | Contraindicated Movements | Safe Guidelines | Responsibility |
|---|---|---|---|
| Spinal stenosis, spondylosis, spondylitis, spondylolysis, spondylolisthesis, herniated disks, arthritis, scoliosis | Excessive spine bending and loading in flexion, rotation, lateral bending, and extension | Start with limited range of motion Progress slowly Avoid training at or near end range of motion Use light to moderate loads | Fitness professionals and exercisers must assess: Safety and efficacy of exercise selection Proper loading (using The RPE Method) Optimal joint range of motion on a case-by-case basis |
Other examples of spine-friendly exercises, assuming proper frequency, volume, intensity, and pain-free range of motion include but are not limited to:
- Deadlifts
The deadlift is a hip-hinge exercise – the torso contracts isometrically and the spine remains stable while the hips are hinging in space. They strengthen the musculature involved in protecting the low back. The exerciser may need to shorten the range of motion, but deadlifts can be a spine-friendly exercise.
- Hip thrust
Hip thrusts are a spine-friendly exercise for the same reason mentioned above with deadlifts.
- Leg press
The leg press is a spine-friendly exercise in most situations because the back is supported, and the torso remains stable.
- Goblet squat and front squat
The goblet and front squat exercises are spine-friendly in most situations because there is minimal forward torso lean and therefore minimal stress on the spine and low back. The spinal erectors and torso are activated. These are muscles which assist in preventing and managing back pain.
- Gluteus medius strengthening exercises
The gluteus medius acts as a hip and pelvis stabilizer. Strengthening this muscle group indirectly assists in preventing and recovering from back pain. Most gluteus medius strengthening exercises involve little to no movement or load on the spine and are normally spine friendly.
For additional clarity on spine-friendly concepts and exercises, view the related video found at www.MRFInstitute.org.
The Shoulder
Chronic or recurrent shoulder discomfort is common, even if people have completed physical therapy for their condition. Examples include “weightlifters’ shoulder,” impingement syndrome, anterior shoulder instability, partial labral tears, and partial rotator cuff tears (Kolber, 2010; Schwartzberg, 2016; Teun, 2014).
To design programs for people who suffer from shoulder pain the fitness professional or individual should understand a concept known as the “shoulder safe zone.” (Cilenti, 2018)
Shoulder Safe Zone
Figure 12.5a: Shoulder Safe Zone in Flexion
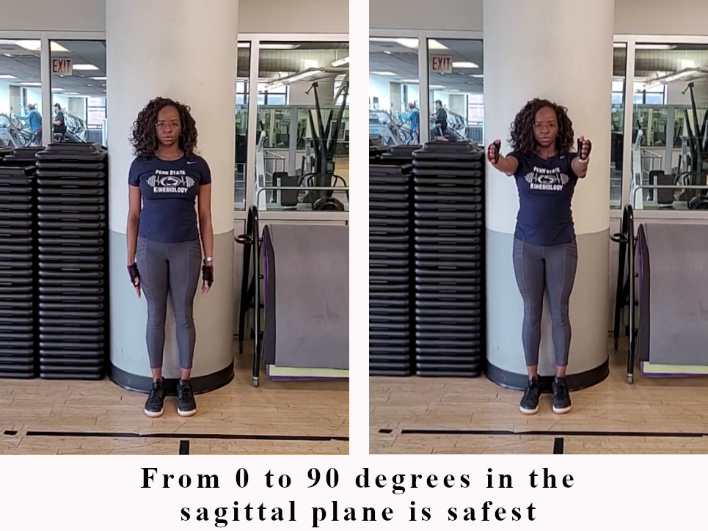
Figure 12.5b: Shoulder Safe Zone in Flexion
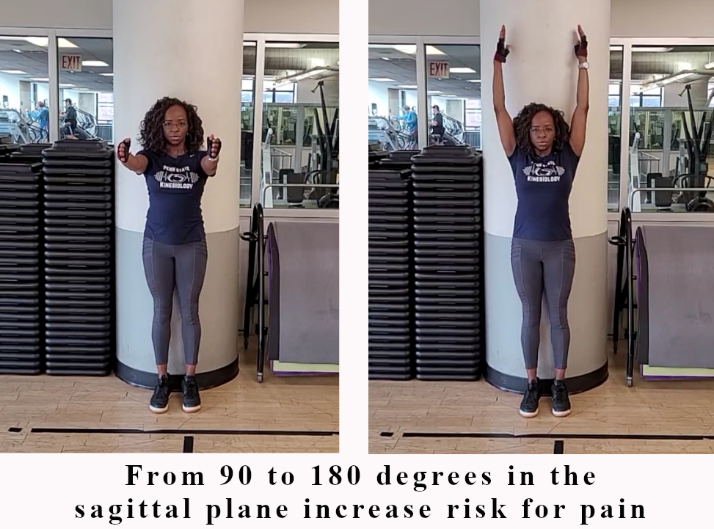
Figure 12.5c: Shoulder Safe Zone in Abduction
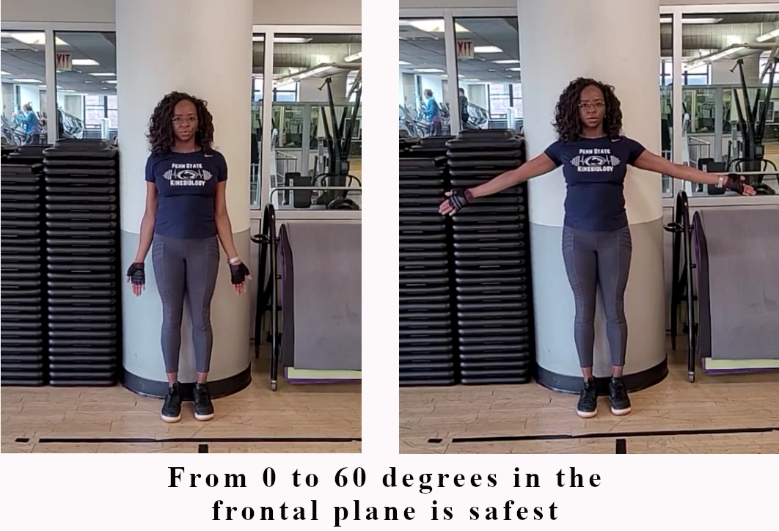
Figure 12.5d: Shoulder Safe Zone in Abduction
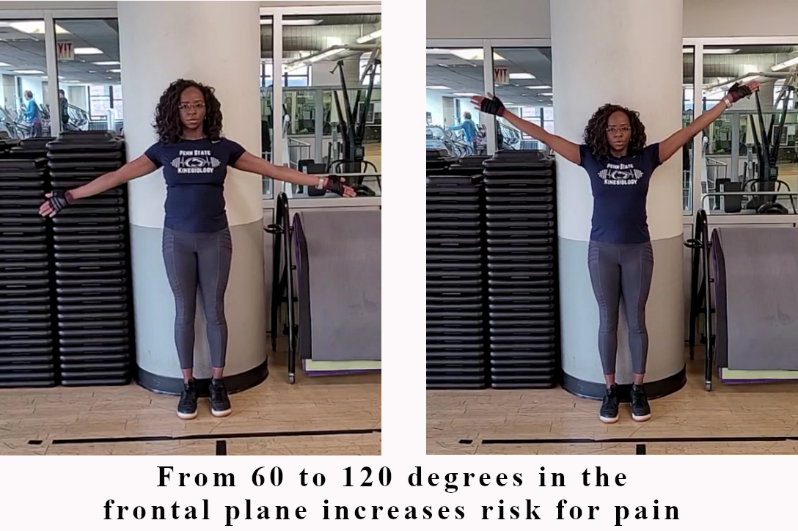
Figure 12.5e: Shoulder Safe Zone in Abduction
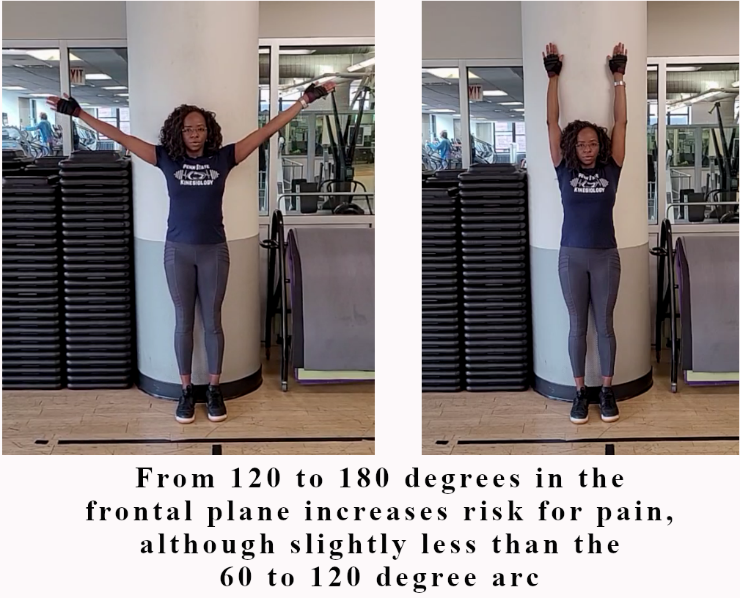
Figure 12.5a represents the safest range of motion for an individual with shoulder pain when the shoulder is moving in the sagittal plane – shoulder flexion. This range is approximately zero to 90 degrees. Figure 12.5b represents an increase in risk of pain, especially when lifting weight. This range is from approximately 90 to 180 degrees (or beyond 180 degrees if the person is hypermobile). Figure 12.5c represents the safest range of motion for an individual with shoulder pain when the shoulder is moving in the frontal plane – shoulder abduction. This range is approximately zero to 60 degrees. Figure 12.5d represents an increase in risk of pain, especially when lifting weight. This range is from approximately 60 to 120 degrees. Figure 12.5e represents an increased risk of pain especially when lifting weight, although slightly less than the 60 to 120 degree arc. This range is approximately 120 to 180 degrees.
Figure 12.5f: Most Vulnerable Shoulder Position
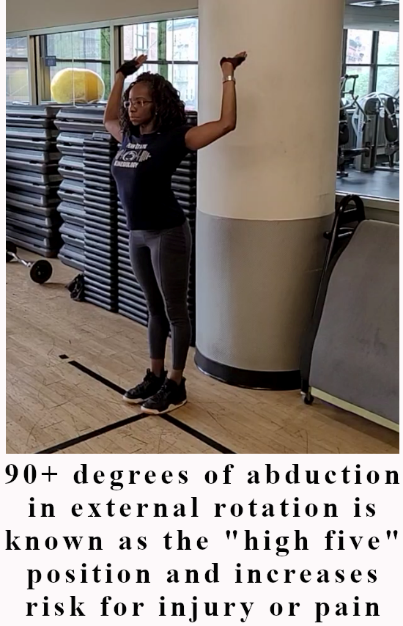
The “high five” position (Figure 12.5f) is the most vulnerable position for the shoulder to be in. In this position the shoulder is abducted at 90 degrees or greater, and is simultaneously externally rotated. This places the shoulder capsule and some of the musculature in a stretch position and should be avoided, as the risk for injury outweighs any benefit (Kolber, 2010).
Movements to Potentially Avoid for Individuals Experiencing Shoulder Pain
Movements that occur within the “safe zone” are typically well tolerated. Although, instances may occur that require limiting or avoiding certain movements in this space too. Depending on the person’s condition and severity of pain, the following movements may need to be initially modified, limited, or eliminated completely.
- Reaching overhead. Examples include:
- - Pull-ups
- - Lat pulldown
- - Overhead press
- Flaring out the upper arm (i.e. shoulders/upper arm abducted) away from the torso, especially beyond 60 degrees. Examples include:
- - Wide grip lat pulldown or seated row
- - Excessive upper arm flare during any chest-press exercise
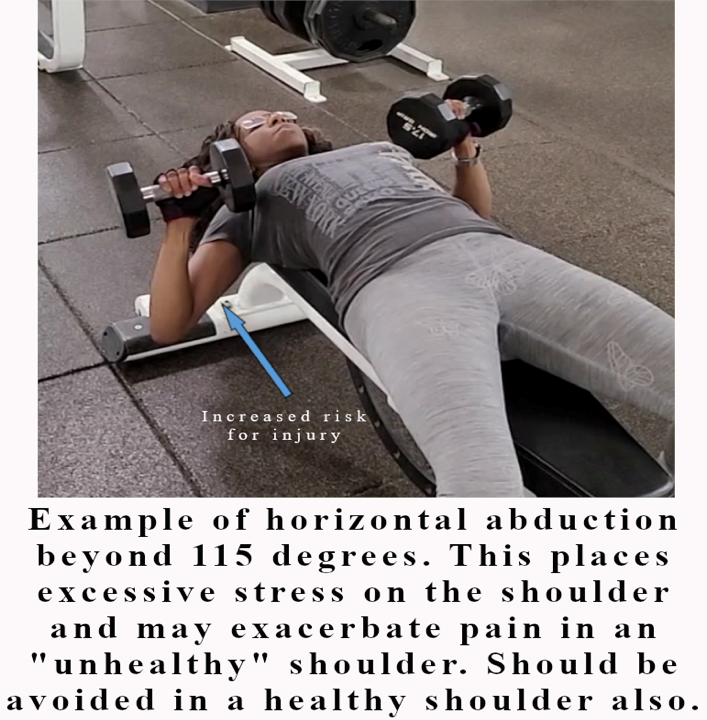
- Excessive depth (i.e. shoulder horizontal abduction beyond approximately 100 to 115 degrees) during any chest exercise/pressing movement (Figure 12.6).
- - An example would be allowing the upper arm to move more than 10 to 15 degrees below the torso (i.e. more than 10 to 15 degrees below parallel to the ground when performing a flat barbell or dumbbell press).
Figure 12.6: Excessive Shoulder Horizontal Abduction.
- Narrow or wide grip bench press,
- - This can place excessive stress on the shoulder capsule, increase the risk for injury, and should either be avoided or programmed sparingly.
- - For some individuals push-ups can place excessive stress on the shoulder capsule (and wrists), especially when the upper arm is flared beyond 60 degrees.
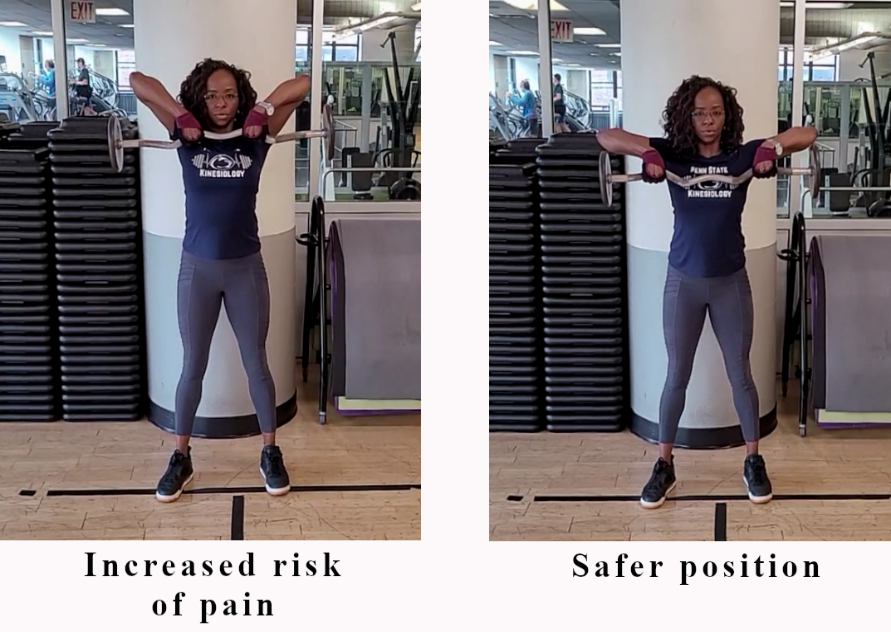
- Close grip upright rows.
- - When the upper arm travels above parallel to the ground (i.e. beyond 90 degrees of abduction) this can greatly increase the risk of shoulder impingement and pain.
- - Wide grip upright rows where the movement is terminated when the upper arm reaches parallel to the ground is a safer choice. These points should be considered when selecting exercises for individuals with shoulder pain (see Figure 12.7).
Figure 12.7: Upright Row Exercise Positions.
Movements to Help Relieve Shoulder Pain
An understanding of the “safe zone” allows the exerciser to select movements or exercises that are safer, and avoid those with a higher risk of causing pain. Exercises that occur in the “safe zone” include:
- Rowing exercises where the lifter does not need to place the arms overhead at any point in the movement or excessively abduct the shoulder at any point in the movement (i.e. the upper arm remains close to the torso during the entire movement). Examples include:
- - Close grip seated row
- - Horizontal cable row
- - Bent-over dumbbell row
- - Bent-over close grip barbell row
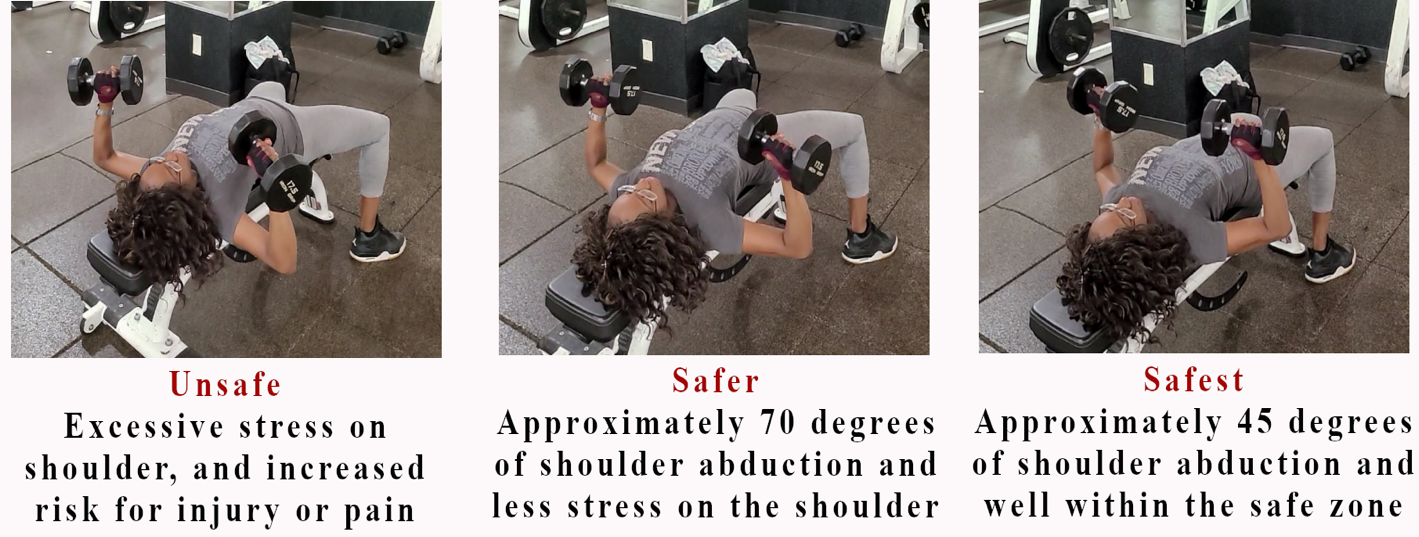
- Chest press exercises where the lifter avoids excessive shoulder abduction (upper arm flare) and excessive shoulder horizontal abduction (too much depth at the end of the movement; see Figure 12.8).
Figure 12.8: Chest Press with Varying Degrees of Shoulder Abduction
- Additional exercises may potentially assist in improving shoulder integrity. To be safe, they should occur within the pain free range of motion and provide an appropriate load. These exercises can include:
- - Lateral raise.
- - Scaptions.
- - Reverse flyes.
- - Face pulls.
- - Rotator cuff strengthening exercises.
For additional clarity on shoulder-friendly concepts and exercises, view the related video found at www.MRFInstitute.org.
The Neck
The neck is in the safest position when:
- The chin is retracted so that the head sits directly over spine (i.e. absent of forward head posture).
- - This normally constitutes a standing or seated position.
- The head is supported and the chin is in a neutral position (i.e. the cervical spine is neither flexed nor extended).
- The upper trapezius is as relaxed as possible during an exercise.
- The scapula are retracted (i.e. absent of sloped/forward shoulder posture).
- Natural shoulder slope is mantained during an exercise (i.e. no “packing” of the neck is occuring), and the neck is as relaxed as possible.
Deviations from the above may place the person who suffers from neck conditions at greater risk for injury or pain (Hansraj, 2014). Examples of movements and exercises that may need to be avoided, at least initially, include:
- Reaching overhead (increases the risk of contracting the upper trapezius or “packing” the neck):
- Lat pulldown.
- Pull-up.
- Overhead press.
- Forward torso lean with head unsupported (increases the risk of sloped shoulder and/or forward head posture):
- Bent-over rows.
- Bent-over reverse flyes.
- Suspension rows, crunches, sit-ups, and planks.
- These exercises allow gravity to pull the head towards the ground. This can lead to a more forceful contraction of neck musculature, and increase the risk that the neck will not be maintained in a neutral position.
Examples of movements and exercises that place the neck at less risk for injury or pain include:
- Any standing or seated exercise where the chin remains in a neutral position; the chin is retracted; natural shoulder slope is maintained; the neck is as relaxed as possible; appropriate load is applied; and proper form is maintained. Examples include:
- Seated and standing rows.
- Standing cable chest press.
- Various seated or standing shoulder strengthening exercises such as lateral raises and scaptions.
- Various seated or standing reverse flye variations such as cable reverse flyes.
- Chest press on a bench.
- Abdominal strengthening exercises lying on the floor, a table, or mat such as Pilates mat exercises.
If an individual is experiencing neck discomfort during an exercise:
- Ensure the chin is retracted.
- Ensure the chin is in neutral position (i.e. neither flexed nor extended).
- Ensure the scapula are retracted.
- Ensure they are maintaining their natural shoulder slope throughout the movement.
- Ensure their neck is as relaxed as possible.
- Place their head and neck in a supported position (e.g. on a mat or bench) with their chin retracted and in neutral, scapula retracted, natural shoulder slope, and relaxed neck.
Cueing and Feedback
In any situation where an individual suffers from musculoskeletal pain, cueing and feedback are of utmost importance. Providing regular feedback using verbal, tactile, and visual cues is important. Feedback should consistently be given to:
- Initiate the movement with the primary mover and focus on consistently using it during the entire set.
- Stay within pain-free available range of motion.
- Adjust angle of the exercise if by doing so pain is alleviated.
- Adjust load if by doing so pain is alleviated.
- Terminate the set if the pain is sharp, stabbing, burning, or the person experiences numbness or tingling.
- - Many times, low-level discomfort such as a dull ache resolves itself with movement because of the secretion of joint fluid or an increase in muscle temperature. If this does not occur quickly or if discomfort increases, the exercise should be terminated.
It is the fitness professional or exerciser’s responsibility to make the appropriate decisions regarding exercise selection, loading, range of motion, and joint angles on a case-by-case basis to determine when adjustments or the termination of a set or exercise is warranted.
For additional clarity on neck-friendly concepts and exercises, view the related video found at www.MRFInstitute.org.
Practical Application Summary
This section consolidates the key principles and strategies outlined in the chapter, offering actionable guidance for fitness professionals and individuals addressing musculoskeletal (MSK) conditions:
- Universal Principles of MSK Program Design
- - Prioritize pain-free movement by adjusting joint angles, ranges of motion, and loads as needed.
- - Focus on the six components of musculoskeletal health: neuromuscular control, strength, strength-endurance, joint stability, posture/alignment, and mobility.
- - Progressively increase strength and conditioning to build resilience and reduce injury risk.
- Condition-Specific Recommendations
- - Knee Pain: Emphasize “knee-friendly” exercises like hip thrusts, deadlift variations, and gluteus medius strengthening. Limit deep knee flexion or forward weight distribution if necessary.
- - Low Back Pain: Start with isometric trunk stabilization exercises before progressing to spinal movement exercises. Avoid excessive spine bending, especially at or near end ranges.
- - Shoulder Pain: Use the “shoulder safe zone” to guide movement. Avoid positions like excessive horizontal abduction or overhead flaring. Focus on controlled, pain-free motions such as rowing and lateral raises.
- - Neck Pain: Maintain neutral head and scapular alignment during exercises. Avoid unsupported head positions or forward torso lean. Focus on seated or supported movements to minimize neck strain.
- Cueing and Feedback
- - Consistently provide verbal, tactile, and visual cues to ensure proper form and movement patterns.
- - Adjust movements, angles, or loads to alleviate pain and terminate sets if sharp or intense pain arises.
- - Encourage slow progression to build confidence and avoid aggravating conditions.
- Holistic Approach to MSK Health
- - Integrate flexibility, mobility, and core strengthening into every program to enhance overall joint and muscle function.
- - Collaborate with healthcare professionals for individuals transitioning from rehabilitation to fitness programs.
By adhering to these principles and tailoring programs to individual needs, fitness professionals can create safe, effective, and comprehensive strategies for managing MSK conditions, promoting long-term health and functionality.
Section 2: General Guidelines and Considerations for Individuals with Osteopenia or Osteoporosis
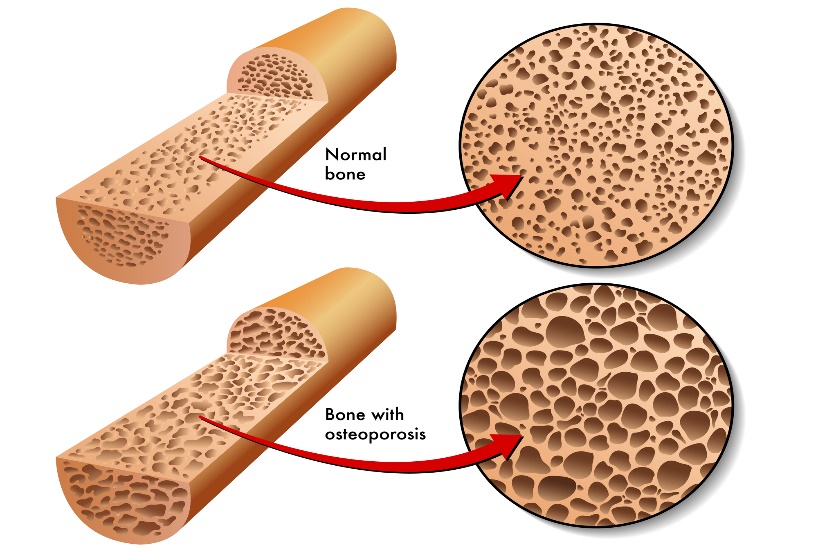
Osteoporosis affects 200 million people worldwide and causes almost nine million fractures every year. Its prevalence increases from age 50 and beyond. Osteopenia and osteoporosis can lead to fractures of the forearm, upper arm (humerus), lumbar spine, hips, and thigh (femur). By 2050, the worldwide incidence of hip fractures in men is projected to increase by 310% and 240% in women, compared to rates in 1990. And most high-risk individuals (possibly 80%) who have had at least one osteoporotic fracture are neither identified nor treated.
Figure 12.9: Normal Versus Osteoporotic Bone
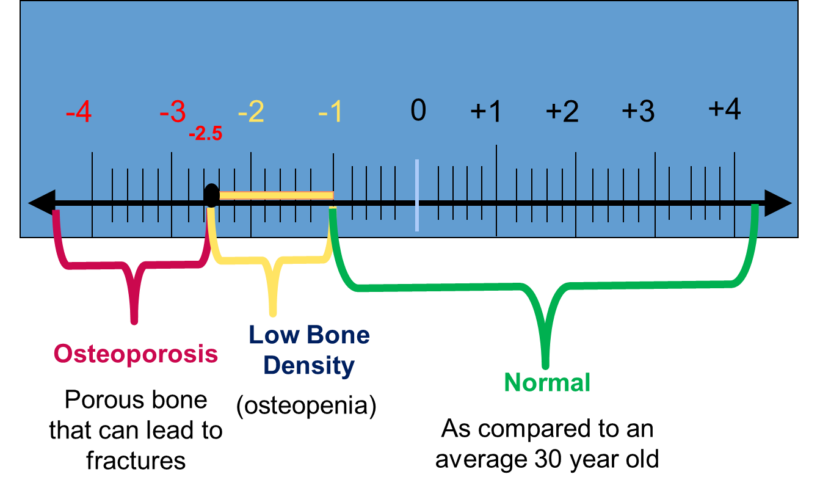
Bone density is categorized into three groups by what is called a T-score (see Figure 12.10).
- Normal – within one standard deviation (SD) of the mean for an average 30-year-old (green area in the chart below). Above one SD means your bones are stronger than the normal adult. For example, a +1 to +2 SD indicates your bones have a mass 10 to 20% above that of the average 30-year-old adult.
- Osteopenia – ranging from 1 to 2.5 standard deviations below the mean for normal adults (yellow area in the chart below). This indicates bone mass is 10 to 25% below that of the average 30-year-old adult. Risk of bone fracture is low to medium.
- Osteoporosis – greater than 2.5 standard deviations below the mean for normal adults (red area in the chart below). For example, a -3 to -4 standard deviation indicates bone mass is 30 to 40% below that of the average 30-year-old adult. Risk of bone fracture is medium to high.
Figure 12.10: Bone Density Standard Deviation Categories (T-Score)
Osteopenia and osteoporosis are largely preventable. Individuals with an active lifestyle and healthy diet are at low risk for developing this condition. Physical activity and exercise serve important roles in preventing, managing, or potentially reversing osteopenia and osteoporosis. General physical activity should be increased as much as possible (Cheatham, 2017; Kohrt, 2009).
As mentioned in Chapter 1, and related to Wolff’s law, heavier loading (e.g., including the 6 to 8 and 4 to 6 repetition ranges in the program design) and varying the angles of push and pull are primary ways to optimize bone adaptations. Both are accomplished within the design of a Flexible Periodization program.
Individuals diagnosed with osteopenia or osteoporosis at the lumbar spine should avoid excessive (i.e., at-or-near end range of motion) flexion, rotation, and lateral bending when performing core-strengthening exercises. They should also remain within a range of motion that is pain free and use only light to moderate loads.
Bone Strengthening with Plyometric Exercise
Studies have shown that plyometric exercise is also beneficial for individuals with osteopenia, and potentially for individuals with early-stage osteoporosis. For safety, the fitness professional should wait until the client has developed strength outside of a beginner domain (i.e., intermediate level). They must also take other conditions into account, such as knee or hip osteoarthritis, or late-stage osteoporosis. In these instances, plyometric exercises would be contraindicated (Cheatham, 2017).
Plyometric exercises should only be incorporated into the exerciser’s program design under the conditions described above, and only after approval from a medical professional.
If the individual can perform plyometric exercises without joint pain, they should begin with low-intensity exercises. This could include short bouts of jump rope or low volume, standing vertical jumps. They should ensure they can do these without any pain or issue before potentially progressing to moderate-intensity plyometric exercises.
Summary
A healthy diet combined with increased general physical activity, a Flexible Periodization program, and appropriately prescribed low to moderate-intensity plyometric exercise are the primary interventions in combatting osteopenia and osteoporosis.
Within the Flexible Periodization program, the exerciser should:
- Recognize the importance of increased loading and varying joint angles to maximize bone strengthening adaptations (Wolff’s law).
- Emphasize revolving programs around primary, compound exercises to optimize bone-strengthening adaptations. Progress to the 4 to 6 repetition range when possible. This should only occur after strength has increased beyond the beginner domain, and only if the T-score is above a -3 SD and there is no bone pain or unhealed fractures.
- Follow the guidelines suggested in this chapter (and corresponding videos) for knee, low back, hip, and neck “friendly” exercises.
- Avoid full range of motion and moderately heavy to heavy loads when having the exerciser perform spine flexion, rotation, and lateral bending.
Initial Exercise Assessments
- Flexibility and trigger point assessment. The fitness professional or exerciser should incorporate the flexibility and trigger point assessments as described in Chapter 7 along with the additional considerations described in Chapter 11.
- Cardiovascular assessment. The fitness professional or exerciser can follow the guidelines in Chapter 5 along with the additional considerations in Chapter 11.
- Strength assessment. The fitness professional or exerciser should incorporate the strength assessment as part of the Familiarization Phase, as described in Chapter 6.
Program Design Considerations
- Cardiovascular program design. People with osteopenia or osteoporosis should engage in aerobic exercise four to six days per week (if possible), 20 to 60 minutes per session, at an RPE of 4 to 6 (on a 1 to 10 scale). The goal is to accrue 150 to 300 minutes of moderate to vigorous intensity aerobic exercise each week (Garber, 2011).
High-intensity interval training (or modified interval training, such as interval walking) can be implemented within training sessions once the person can maintain 20 minutes or greater of continuous aerobic exercise at an RPE of 5 to 6 (Ribeiro, 2017). If high-intensity exercise is implemented within the program:
- Overall volume/duration should be low (i.e. cycle through the recovery:work period no more than three times and progress from there).
- The work portion should be relatively short (e.g., 30 to 60 seconds).
- The recovery portion should begin at a 3:1 to 5:1 rest to work ratio (e.g., 120 seconds of rest for every 30 seconds of work).
- The intensity should primarily be guided via the use of the RPE-Talk Test method.
- The program should begin with modified high-intensity interval training (i.e., interval walking program) for more deconditioned individuals, whereby the work portion remains in the moderate to high end of the aerobic training zone for a short period as opposed to the anaerobic training zone.
Impact exercise (e.g., walking or jogging) should be incorporated more often than non-impact (e.g., swimming, cycling, elliptical machine) exercise, unless the person has bone pain, joint pain, or unhealed fractures. In this case, impact aerobic exercise may need to be modified or avoided. See Chapter 5 for more information on cardiovascular assessment and program design.
Table 12.2: Example Cardiovascular Program Design
Table 12.2: Example Cardiovascular Program Design
| Day | Duration (Minutes) | Intensity (RPE-Talk Test method) |
|---|---|---|
| Monday | 20 to 60 | 4 to 6 RPE |
| Tuesday | 20 to 60 | 4 to 6 RPE |
| Wednesday | 10 to 15 | *Modified high-intensity interval training |
| Thursday | 20 to 60 | 4 to 6 RPE |
| Friday | 20 to 60 | 4 to 6 RPE |
- Including a modified high-intensity interval training session is at the fitness professional or exerciser’s mutual discretion. It should be based on fitness level, absence of symptoms, well-controlled resting blood pressure, and having a positive response to exercise progression. The recovery portion should be at an RPE of 2 to 3 and work portion at an RPE of 6 to 7.
- - For example, recovery to work ratio may begin at 5:1 or 6:1, cycling through each ratio 3 to 5 times (e.g., 2.5 minutes at an RPE of 2 to 3 followed by 30 seconds at an RPE of 6 to 7); see RPE-Talk Test method in Chapter 6 for more detail).
- It is the fitness professional or exerciser’s responsibility to determine frequency, duration, intensity, and progression on a case by case and session by session basis.
- Resistance training program design. The exerciser can follow the resistance training guidelines covered in Chapters 4 and 6 with the following additional considerations:
- - Always ensure “readiness to train” questions are asked prior to every session. Based on the answers to each question, the volume and intensity of the session should be adjusted accordingly.
- - If the person begins to develop any of the following symptoms: light-headedness, dizziness, nausea, pale or clammy skin, excessive sweating, headache, chest pain, chest tightness, heart palpitations, unusual fatigue, blurred vision, or feels anything “other than the norm,” terminate the session and seek medical advice.
- - Avoid exercises where the spine is taken to at or near “end range” in flexion (e.g., sit-ups), rotation, or lateral bending (e.g., oblique raises), especially under moderate to heavy loads if the person has been diagnosed with osteopenia or osteoporosis at the lumbar spine.
- - Following the low volume, low intensity Familiarization Phase, use The RPE Method as the primary guide for intensity adjustments. Working sets should be terminated when the RPE reaches a 6 to 8 on a 1 to 10 scale.
- - If the person’s T-score is below -3, avoid training in the 1 to 4 repetition range. Plyometric exercises should also be avoided. It is best to consult with a medical professional to seek additional advice regarding exercise restrictions and contraindications.
Table 12.3: General Flow of a Resistance Training Session
Table 12.3: General Flow of a Resistance Training Session
| Exercise | Intensity |
|---|---|
| Always begin with Readiness to Train questions and adjust or terminate sessions appropriately and accordingly | |
| Trigger Point Release | Low |
| Dynamic Warm-up | Low to Moderate |
| Core Warm-up | Low to Moderate |
| Total Body Workout | Use The RPE Method |
Table 12.4: General Scope of a Week
Table 12.4: General Scope of a Week
| Weekly Scope |
|---|
| Vary Intensities from low to moderately high or high using The RPE Method |
Table 12.5: General Set-up of a Flexible Linear Periodization Model
Table 12.5: General Set-up of a Flexible Linear Periodization Model
| Phase | Length of Phase | Intensity (The RPE Method) |
|---|---|---|
| Familiarization (initial program design) | As needed. Typically, 3 to 8 weeks. | 4 to 6 RPE |
| 12 to 15 repetitions per set | 3 to 4 weeks | 6 to 7 RPE |
| 10 to 12 repetitions per set | 3 to 4 weeks | 6 to 7 RPE |
| 8 to 10 repetitions per set | 3 to 4 weeks | 6 to 8 RPE |
| 6 to 8 repetitions per set | 2 to 3 weeks | 6 to 8 RPE |
Note: It is the fitness professional or exerciser’s responsibility to determine repetition ranges, phase lengths, and session intensities on a case by case, session by session basis.
Practical Application Summary
This section consolidates the key principles and strategies for designing exercise programs for individuals with osteopenia and osteoporosis, offering actionable guidance for fitness professionals and exercisers:
General Guidelines
- Increase Physical Activity: Encourage a combination of general physical activity and structured exercise to promote bone health and reduce fracture risk.
- Flexible Periodization Program: Incorporate progressive strength training with increased loading (4–6 repetition range) and varying joint angles to maximize bone-strengthening adaptations (Wolff’s law).
- Spine-Specific Precautions: Avoid excessive flexion, rotation, or lateral bending at or near the spine’s end range, especially under moderate to heavy loads.
Cardiovascular Program Considerations
- Frequency and Duration: Aim for 4–6 sessions per week, accumulating 150–300 minutes of moderate to vigorous aerobic exercise at an RPE of 4–6.
- Impact Exercise: Prioritize weight-bearing activities like walking or jogging, unless contraindicated by joint pain or fractures.
- High-Intensity Interval Training (HIIT): Implement modified HIIT cautiously, starting with a 3:1 to 5:1 recovery-to-work ratio and progressing based on the individual’s fitness level and symptom response.
Resistance Training Considerations
- Readiness to Train: Evaluate the exerciser’s readiness before each session, adjusting intensity and volume as needed.
- Progressive Loading: Start with low volume and intensity, progressively increasing based on individual tolerance and strength assessments.
- Plyometric Training: Introduce low-intensity plyometrics only when the individual has surpassed beginner strength levels and is free of contraindications.
Safety Precautions
- Contraindications: Avoid heavy loads, full range of motion in spinal movements, and plyometric exercises for individuals with severe osteoporosis (T-score below -3) or unhealed fractures.
- Monitoring Symptoms: Terminate sessions if symptoms such as dizziness, chest pain, or unusual fatigue occur, and consult a medical professional when necessary.
Practical Implementation
- Structured Weekly Plan: Use a flexible linear periodization model with varied intensities and repetitions (e.g., 6–8 RPE, 6–8 repetitions) tailored to the individual’s needs and progress.
- Holistic Assessments: Incorporate flexibility, cardiovascular, and strength assessments to ensure a balanced approach.
Key Takeaway
By adhering to these principles, fitness professionals can design safe and effective programs that enhance bone health, improve physical function, and minimize fracture risk in individuals with osteopenia or osteoporosis.
Chapter 12 Summary: Integrating MSK and Osteoporosis Program Design
This chapter underscored the integral role of tailored exercise programming in managing and improving musculoskeletal health and osteoporosis. For MSK conditions, the outlined universal principles—focusing on mobility, strength, joint stability, and proper form—serve as a foundational approach applicable across a range of conditions, including knee, back, shoulder, and neck pain. By adhering to a structured and progressive program, individuals can achieve better movement efficiency, reduced pain, and increased resilience against injury.
In addressing osteoporosis, the chapter emphasized safe yet effective exercise protocols to enhance bone density and reduce fracture risk. Specific guidelines for resistance, balance, and mobility training highlighted the balance between promoting skeletal strength and avoiding potentially harmful movements.
By integrating these guidelines into comprehensive fitness programs, practitioners can effectively bridge the gap between rehabilitation, fitness, and long-term health. This holistic approach empowers individuals to achieve sustained improvements in both musculoskeletal integrity and overall functional capacity.