Full chapter reading
Chapter 10: Nutrition
While nutrition often stands apart from exercise programming, its integration into the universal algorithm ensures that dietary strategies support and enhance fitness outcomes. A basic understanding of nutrition principles can make an enormous difference in the perceived effectiveness of a program. It is particularly relevant for individuals wanting to perform at high levels, add significant muscle mass, or lose body fat. Without achieving the appropriate energy balance through diet and exercise with these individuals, they will be unlikely to achieve their goals.
When discussing nutrition with clients, it is important to ensure that the fitness professional is acting within their scope of practice. General recommendations and offering feedback or guidance surrounding healthier food choices is generally acceptable. However, detailed dietary instruction or more extreme versions of diets should be left to dieticians and health professionals. Fitness professionals may have a larger scope of practice depending on the state but should always operate within their purview.
The field of nutrition can seem confusing, conflicting, and controversial; however, it does not have to be. The biggest challenge is clearly defining the goal trying to be accomplished with the diet. For example, a diet that optimizes muscle hypertrophy will look different from one that is designed for weight loss. This chapter will review some of the fundamental aspects of nutrition, introduce the different energy systems, and offer general nutrition recommendations that can be tailored to clients depending on their activity level, goals, and dietary preferences.
What is food?
Food is fundamentally a source of energy and provides the substance for tissue growth and repair. We quite literally become the food we consume. At an elemental level, everything we eat is a combination of carbon, hydrogen, oxygen, and nitrogen, with trace amounts of other elements (i.e., vitamins and minerals). These elements are combined in numerous ways to create three macronutrients: protein, fat (lipids), and carbohydrates (carbs, CHOs). Within each of these macronutrient categories, there are specific types of proteins (made up of various combinations of amino acids), fats (monounsaturated, polyunsaturated, saturated fats, etc.), and carbohydrates (simple and complex).
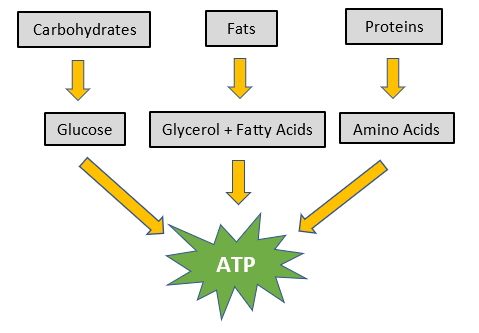
Once consumed, carbohydrates, fats, and protein are broken down to glucose, free-fatty acids, and amino acids, respectively. Most of these glucose and free-fatty acids, as well as some amino acids, will ultimately be converted to Adenosine Triphosphate (ATP) (Figure 10.1). This ATP is considered the universal energy "currency” of the body and is used in virtually all metabolic processes, including muscle contraction. Understanding the role that carbohydrate, fat, and protein play in these processes, and potential benefit of each of these compounds can help guide dietary recommendations for individuals.
Figure 10.1: Macronutrient Digestion.
Food should not be viewed as “good” or “bad;” however, depending on the specific food molecule, it can have effects on the body that can improve or worsen health.
The Three Major Energy Systems
Depending on much and how quickly energy is needed, the body will use different energy systems. The three primary energy pathways are the Phosphagen (ATP-PC; Anaerobic), Glycolysis (Anaerobic), and Oxidative Phosphorylation (Aerobic). Carbohydrates and fat are the predominant fuel sources for energy. Protein or amino acids can provide some energy, but in general, protein is preferentially spared when adequate fat and carbohydrate are available for energy. Table 10.1 summarizes the energy systems.
Table 10.1 Energy System Summary.
Table 10.1: Energy System Summary
| Energy System | Recruitment & Duration of Action | Primary Energy Source |
|---|---|---|
| Phosphagen (ATP-PC; Anaerobic) | Immediate (10-15 seconds) | Creatine Phosphate |
| Glycolytic (Anaerobic) | Fast (>15-120 or 180 seconds) | Carbohydrates |
| Oxidative Phosphorylation (Aerobic) | Slow (>2-3 minutes) | Fats, Carbohydrates |
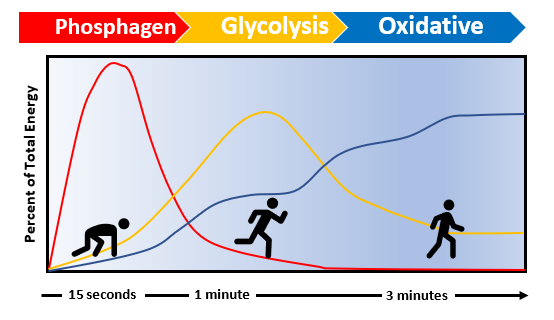
At the onset of exercise, the Phosphagen system provides the majority of ATP. This energy is available immediately. However, there is only sufficient capacity to power activity for 10-15 seconds. If activity continues beyond this brief window, Glycolysis (or Anaerobic) becomes the predominant energy system. Glycolysis (-lysis = break down) takes longer than the Phosphagen pathway because it involves breaking down glycogen to create ATP. Beyond two to three minutes of activity, Oxidative Phosphorylation (or Aerobic) supplies most of the energy. Figure 10.2 summarizes the percentage of energy supplied by each energy system relative to the length of time exercising.
Figure 10.2: Predominant Energy System Used by a Runner from the Starting Blocks of a Race Over Time.
Macronutrient Overview
The following sections will briefly review the relevance and importance of each of the primary three macronutrients: protein, fat, and carbohydrates. Each section will discuss the different types of macronutrients and will provide general recommendations for providing dietary advice. Again, diets should be individualized based on a person’s activity level, goals, and dietary preferences.
Protein
Protein is arguably the most important macronutrient. It is made up of various combinations of 20 amino acids, 9 of which are essential and must be consumed in the diet (Table 10.2). The other 11 amino acids are also needed, but the body has the necessary enzymes to create or convert other amino acids into these.
Table 10.2: Essential and Non-Essential Amino Acids (Allowances., 1989).
Table 10.2: Essential and Non-Essential Amino Acids (Allowances., 1989).
| Essential Amino Acids | Non-Essential Amino Acids |
|---|---|
| Histidine | Alanine |
| Isoleucine | Arginine |
| Leucine | Asparagine |
| Lysine | Aspartate |
| Methionine | Cystine |
| Phenylalanine | Glutamate |
| Threonine | Glutamine |
| Tryptophan | Glycine |
| Valine | Proline |
| Serine | |
| Tyrosine |
Skeletal muscle growth and repair is reliant on having sufficient protein available. The body recycles much of the protein it already has in order to build or re-build tissue as it is damaged. However, dietary protein is needed to build additional muscle and to repair muscle fibers that are damaged with exercise. Protein has 4 kcal (Calories) of energy per gram.
How much protein should be consumed?
Depending on the population of interest and their goals, recommended protein intake varies. For sedentary adults, the US and Institute of Medicine’s (IOM) Recommended Daily Allowance (RDA) for protein is 0.8 g/kg/day, for healthy adults (Medicine, 2005). The International Society of Sports Nutrition position stand states that protein intakes between 1.2 to 2.0 g/kg/day will likely suffice for the general population, depending on the goals (Campbell, 2007). These general recommendations are likely sufficient for the general population, however, they may not be optimal for individuals trying to increase muscle mass and strength. Optimizing these outcomes and combating age-related muscle mass loss (i.e. sarcopenia) requires a slightly higher protein intake than these general recommendations (Paddon-Jones, 2009) (Schoenfeld B. A., 2018).
A 2018 review article concluded that anabolism (i.e. muscle building) was maximized by consuming 1.6 to 2.2 g/kg/day of protein. Their suggestion was to divide this across four meals, necessitating 0.4 to 0.55 g/kg/meal (Schoenfeld B. A., 2018) Table 10.3 provides the recommended total and per meal protein intake based on body weight.
No good evidence exists that protein intake beyond the upper limit of 2.2 g/kg/day provides any additional benefit. Furthermore, protein intakes beyond this may increase protein conversion into energy. One exception to the above recommendations is patients with renal disease. Protein is filtered by the kidneys, so these individuals should consume a low-moderate protein diet in the 0.8 to 1.2 g/kg/day range (Campbell, 2007; Friedman, 2004; (Schwingshakl, 2014).
Table 10.3: Recommended Protein Intake per Day/Meal Based on Body Weight.
Table 10.3: Recommended Protein Intake per Day/Meal Based on Body Weight.
| Pounds | Kilogram | Total Daily Protein (g) at 1.6 g/kg/day | Protein per Meal (4 meals) at 1.6 g/kg/day | Upper Limit Total Daily Protein (g) at 2.2 g/kg/day | Upper Limit Protein per Meal (4 meals) at 2.2 g/kg/day |
|---|---|---|---|---|---|
| 100 | 45 | 73 | 18 | 100 | 25 |
| 125 | 57 | 91 | 23 | 125 | 31 |
| 150 | 68 | 109 | 27 | 150 | 37 |
| 175 | 79 | 127 | 32 | 175 | 44 |
| 200 | 91 | 145 | 36 | 200 | 50 |
| 225 | 102 | 163 | 41 | 224 | 56 |
| 250 | 113 | 181 | 45 | 249 | 62 |
To optimize muscle growth and maintenance, the authors recommend consuming 1.6 g/kg (~0.8 g/lb) of protein per day, ideally split across four meals.
Protein Quality
Significant confusion exists regarding the “quality” of different proteins. Historically, the literature has referred to some proteins as “complete” or “incomplete.” This distinction creates an inaccurate understanding of protein, amino acids, and food.
ALL dietary protein includes all 20 amino acids. However, the proportion of specific amino acids varies depending on the food.
For example, eggs are considered a “complete” protein and frequently the standard to which other proteins are compared with. Eggs, and most animal derived proteins have all 20 amino acids. More importantly though, they have high proportions of the essential amino acids. The term “complete” was meant to indicate that high proportions of all essential amino acids were available.
Incomplete proteins also have all 20 amino acids but may have low quantities of certain essential amino acids. This resulted in the notion of needing to combine foods. For example, rice and beans are both considered “incomplete” protein sources, despite having all 20 amino acids. They each have relatively lower amounts of certain amino acids. However, when consuming the food together, their individual amino acid profiles complement one another, resulting in sufficiently high levels of all essential amino acids. Although all proteins are considered “complete,” in the sense that they contain all amino acids, plant derived proteins are generally best when combined with foods that have complimentary amino acid profiles to ensure that sufficient levels of essential amino acids are consumed. Table 10.4 and Figures 10.3A, B, and C provide a clear illustration of the amino acid concept comparing beans, rice, beans plus rice, and eggs to the RDA. Eggs are often considered a “gold standard” blend of amino acids, so it is helpful to see how the amino acid profiles of plant-based foods compare and how they relate to the recommended allowances. It is important to recognize that the tables and figures have all been standardized to 100 grams of each food.
Table 10.4: Essential Amino Acid Composition of Eggs versus Beans and Rice.
Table 10.4: Essential Amino Acid Composition of Eggs versus Beans and Rice.
| Essential Amino Acid | Beans | Rice | Beans + Rice | Egg | RDA |
|---|---|---|---|---|---|
| Lysine | 714 | 257 | 971 | 1001 | 2100 |
| Histidine | 303 | 165 | 468 | 322 | 700 |
| Threonine | 428 | 246 | 674 | 674 | 1050 |
| Cysteine + Methionine | 238 | 257 | 495 | 740 | 1050 |
| Valine | 616 | 438 | 1054 | 896 | 1820 |
| Isoleucine | 556 | 306 | 862 | 741 | 1400 |
| Leucine | 885 | 590 | 1475 | 748 | 2730 |
| Phenylalanine + Tyrosine | 963 | 588 | 1551 | 1247 | 1750 |
| Tryptophan | 113 | 84 | 197 | 228 | 280 |
Figure 10.3A: Amino Acid Composition per 100 grams of Beans & Rice.
Figure 10.3A: Amino Acid Composition per 100 grams of Beans & Rice
| Essential Amino Acid | Beans | Rice |
|---|---|---|
| Lysine | 714 | 257 |
| Histidine | 303 | 165 |
| Threonine | 428 | 246 |
| Cysteine + Methionine | 238 | 257 |
| Valine | 616 | 438 |
| Isoleucine | 556 | 306 |
| Leucine | 885 | 590 |
| Phenylalanine + Tyrosine | 963 | 588 |
| Tryptophan | 113 | 84 |
Figure 10.3B: Amino Acid Composition per 100 grams of Eggs
Figure 10.3B: Amino Acid Composition per 100 grams of Eggs
| Essential Amino Acid | Egg |
|---|---|
| Lysine | 1001 |
| Histidine | 322 |
| Threonine | 674 |
| Cysteine + Methionine | 740 |
| Valine | 896 |
| Isoleucine | 741 |
| Leucine | 748 |
| Phenylalanine + Tyrosine | 1247 |
| Tryptophan | 228 |
Figure 10.3C: Recommended Daily Allowance (RDA) of Amino Acids
Figure 10.3C: Recommended Daily Allowance (RDA) of Amino Acids
| Essential Amino Acid | RDA |
|---|---|
| Lysine | 2100 |
| Histidine | 700 |
| Threonine | 1050 |
| Cysteine + Methionine | 1050 |
| Valine | 1820 |
| Isoleucine | 1400 |
| Leucine | 2730 |
| Phenylalanine + Tyrosine | 1750 |
| Tryptophan | 280 |
Recognizing that all amino acids are available in any food containing protein allows the fitness professional and client to create a tailored plan that honors the client’s dietary preferences (i.e., Low Carb, Mediterranean, Paleo, Plant-Based, Vegan, etc.), while ensuring that protein and caloric needs are met.
Protein Timing:
A commonly held view within the bodybuilding world is the notion of an “anabolic window” of opportunity post-workout (Aragon, 2013). This was based on research that demonstrated an increase in muscle protein synthesis with early post-workout protein intake (specifically, protein high in the amino acid Leucine) (Phillips, 2011) (Levenhagen, 2001). While this acute process is increased, it has not consistently translated into increased muscle strength or hypertrophy in the long run. A 2013 meta-analysis (considered the highest level of evidence) article of the available literature found that when controlling for potential confounders, there were no significant differences on muscle strength or hypertrophy based on when protein was consumed (Schoenfeld B. A., 2013).
Rather than the timing of consuming protein, the biggest predictor of muscle hypertrophy was total protein intake.
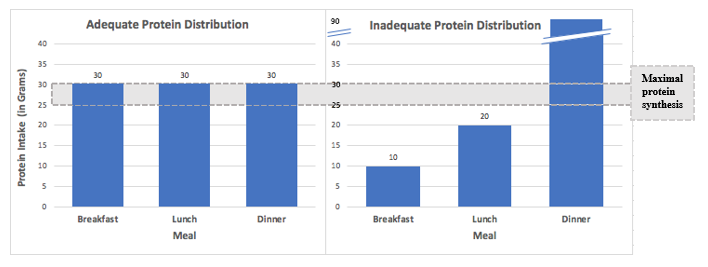
While there is little harm in consuming protein immediately post-workout, it need not be a point of emphasis for most people. Rather, time is better spent educating them on the importance of consuming sufficient protein across the day. Ideally, dividing up protein consumption across three to four meals, aiming for ~25-30 grams (Paddon-Jones, 2009). This helps to maximize protein synthesis over the course of a day.
Figure 10.4: Preferred Protein Distribution (Adapted from Paddon-Jones, 2009).
Meeting this protein requirement can be in the form of whole foods and does not require supplementation. The added benefit of consuming combinations of whole foods is that protein digestion and absorption is delayed, providing an anabolic effect for 3-6 hours after the food is ingested (Layman, 2004) (Atherton). For example, a meal eaten 1-2 hours prior to training will still exert anabolic effects post-workout, negating the need for additional protein until 1-2 hours post-workout. However, when training is initiated more than ~3-4 hours after the preceding meal, consuming protein as soon as possible post-workout makes sense to reverse the catabolic state (Aragon, 2013). Depending on when and if the person ate prior to exercising can dictate how much and when any post-workout protein should ideally be consumed.
The recommendation is for individuals to get their protein from whole food sources, when possible.
If individuals are consistently unable to meet their total protein needs through diet alone, protein supplementation can be added. Protein supplementation may also be appropriate for high level athletes, bodybuilders, or individuals who train multiple times per day. For the theoretical benefit in these groups of individuals, including a protein supplement pre- or post-workout may make sense.
Fat
There is no US or IOM RDA for fat intake, though the Acceptable Macronutrient Distribution Range (AMDR) is typically 20-35% of total calories (Rodriguez, 2013)(IOM, 2005). The IOM actually states that “A Tolerable Upper Intake Level (UL) is not set for total fat because there is no defined intake level of fat at which an adverse effect occurs (IOM, 2005).” Sufficient fat intake is needed to ensure that essential fatty acids are consumed, adequate fat-soluble vitamins are obtained, and weight is appropriately maintained. Fats can be classified as unsaturated fatty acids, saturated, trans fatty acids. The unsaturated fatty acids can be further divided into monounsaturated, polyunsaturated (Table 10.5). Fat has 9 kcal (Calories) of energy per gram.
Table 10.5: Fat Types.
Table 10.5: Fat Types.
| Fat type | Examples |
|---|---|
| Unsaturated Fatty Acids | Examples |
| Monounsaturated | Avocado, Nuts, Olive Oil |
| Polyunsaturated | |
| Omega-3 | Salmon, Walnuts, Flaxseed |
| Omega-6 | Vegetable Oils |
| Trans* | Fried Fast Foods, Bakery Products, Beef |
| Saturated Fatty Acids | Examples |
| Saturated | Butter, Full-Fat Dairy Products, Red Meat |
*Trans fatty acids are technically polyunsaturated fatty acids but for the sake of simplicity, we will consider them as a separate category from polyunsaturated fatty acids
Unsaturated fatty acids include both monounsaturated fatty acids (MUFAs) and polyunsaturated fatty acids (PUFAs)*. These should be the predominant types of fat consumed in the diet.
Monounsaturated fatty acids are characterized by a single (mono-) double bond in their chemical structure and are staples in the Mediterranean diet. They are commonly found in foods such as nuts and olive oil. Their health benefits are well documented, particularly as it pertains to cardiovascular disease and diabetes (Aune, 2016) (Estruch, 2018) (Garg, 1998) (Guasch-Ferre, 2017).
Polyunsaturated fatty acids have more than one (poly-) double bond in their structure and are the only “essential” fats for humans. The two essential fatty acids are an omega-3 fatty acid called alpha-linolenic acid found in salmon, walnuts and flaxseed, and an omega-6 fatty acid called linoleic acid that is found primarily in vegetable oils. Diets tend to include excess amounts of omega-6 fatty acids but are often insufficient in omega-3s (unless people consume multiple servings of fatty fish such as salmon weekly). Multiple meta-analyses have been conducted demonstrating the benefit of omega-3 fatty acids on cardiometabolic diseases (Bucher, 2002) (Hartweg, 2007) (Jang, 2020).
Trans fatty acids are also polyunsaturated fatty acids, but unlike the other polyunsaturated fatty acids they have no health benefits and are fairly detrimental to health. Small amounts of trans fatty acids occur naturally beef and some animal products, they were previously found in fried fast foods and bakery products. They should not be consumed, as research has been shown that that worsen cholesterol levels and increase rates of cardiovascular disease (de Souza Russell, 2015) (Zhu, 2019). The evidence was compelling enough that they were banned in the US in 2015.
Saturated fatty acids do not have any double bonds in their hydrocarbon chain and are solid at room temperature. High levels are found in butter, full-fat dairy, red meat, etc. Most dietary recommendations suggest getting <10% of total calories from saturated fat (Frank, 2106) (Wang, 2016), although there is equivocal evidence on their impact on overall health (de Souza Russell, 2015, Dehghan, 2017, Zhu, 2019).
How much fat should be consumed?
Dietary fat should come primarily from foods that are high in unsaturated fatty acids, with particular emphasis on foods higher in monounsaturated and omega-3 fatty acids. Foods higher in saturated fat should be consumed in moderation, and trans fatty acids should generally not be consumed. Depending on the person’s goals, phase of training, underlying physiology, and dietary preferences, the proportion of fat in the diet can vary.
We recommend that fat intake be tailored to the individual, with 20-35% of total calories serving as a starting point.
Carbohydrates
The US and IOM’s RDA for carbohydrates is 130 g/day, though they acknowledge that this level of carbohydrate intake is typically exceeded to meet energy needs (Institute of Medicine, 2005). Carbohydrates typically make up the majority of an individual’s caloric intake unless they are following a specific dietary plan. They can be categorized as simple carbohydrates and complex carbohydrates. Simple carbohydrates consist of monosaccharides (mono = one, saccharide = sweet; single sugar unit) and disaccharides (di = two; two connected sugar units). Complex carbohydrates include oligosaccharides (oligo = few; three to 10 linked sugar units), and polysaccharides (poly = many; connected sugar units). Oligosaccharides will be considered polysaccharides for simplicity. Carbohydrates have 4 kcal (Calories) of energy per gram, though certain fibers have less. Examples of the different carbohydrates can be found in Table 10.6.
Table 10.6: Carbohydrate Types.
Table 10.6: Carbohydrate Types.
| Carbohydrate type | Examples |
|---|---|
| Simple Carbohydrates | Examples |
| Monosaccharides | Fructose, Glucose, Galactose, Ribose |
| Disaccharides | Lactose, Maltose, Sucrose |
| Complex Carbohydrates | Examples |
| Polysaccharides | Cellulose, Glycogen, Starch |
The body tends to convert all carbohydrates into glucose, which is preferentially used by the brain. It is also an ideal source of fuel for muscle contraction since it can quickly be broken down into ATP. Glucose is stored in skeletal muscle and the liver as glycogen (a polysaccharide). In a normal fed state, there is ~500 g of glycogen (2,000 Calories) stored in skeletal muscle and ~110 g (440 Calories) stored in the liver, totaling ~2,400 Calories (Melzer, 2011). The body closely regulates the amount of glucose circulating in the blood (i.e., blood glucose or blood sugar). It will store excess blood glucose as glycogen or adipose (fat), and if blood glucose levels begin to fall, it will break down glycogen stores into glucose to increase them.
Are all carbohydrates created equal?
The structure and properties of the various carbohydrate types have important implications on what happens metabolically once they are consumed. The body seeks homeostasis--stable blood sugar levels without significant spikes or changes. Simple sugars tend to be broken down and absorbed quickly. This results in a rapid increase in blood sugar, which requires a large amount of insulin to be released to lower it back into the normal range. The rapid rise often leads to the body releasing more insulin than necessary (i.e., it overshoots), which ironically results in blood sugar levels being lower than they were before consuming the simple carbohydrates. This can create a roller coaster of high, and subsequently low blood sugar levels, which can cause long term health issues and increase hunger in the short term.
Consuming complex carbohydrates results in slower digestion and absorption of energy. Blood sugar levels will show less variability, avoiding the highs and lows seen with simple carbohydrates. This provides more sustained energy. Dietary fiber, both soluble and insoluble fiber, is only found in complex carbohydrates. These fibers can aid in blood glucose management, serve as fuel for the “gut” microbiome (bacteria), help with weight management, and decrease Low Density Lipoprotein (LDL) cholesterol levels (Bozzetto, 2018) .
When carbohydrates are consumed, they should ideally be complex.
How much carbohydrate should be consumed?
As stated above, most individuals should consume a minimum of 130 g/day (520 calories). Although reducing carbohydrates can be helpful for weight loss and blood glucose control, it may negatively impact performance. Carbohydrates are the preferred fuel source for higher intensity or anaerobic (without oxygen) activity. Resistance training is heavily reliant on carbohydrates for fuel, as most sets last less than 60 seconds. Therefore, having sufficient carbohydrate intake is necessary if optimizing anaerobic physical performance is the goal.
Carbohydrate intake becomes increasingly important as training frequency increases. For athletes who are training every day or having multiple sessions in a single day, adequate and timely replenishment of carbohydrate and glycogen levels becomes critical. These athletes may need up to 6-10 g/kg/day of carbohydrates to meet their energy demands (Rodriguez, 2013). This may necessitate that carbohydrates be consumed during and immediately post-workout, in addition to throughout the day. Elite endurance athletes may benefit from consuming 1-1.2 g/kg of carbohydrates immediately after exercise (within 30 minutes) (Rodriguez, 2009). This high carbohydrate only becomes relevant with extended aerobic training (>60 minutes) and is usually unnecessary during typical resistance training sessions.
Depending on how active the individual is, and how sensitive their body is to glucose and insulin, complex carbohydrates can make up a substantial portion of the diet. However, For the general population, carbohydrate intake should be matched to their activity level and ability to effectively utilize carbohydrates. Individuals with early signs of insulin resistance, diabetes, or those trying to lose weight, diets lower in carbohydrate may be ideal.
In terms of what types of carbohydrate containing foods to consume, the preponderance of data suggests that higher consumption of vegetables and fruits is health promoting (Wang X. O., 2014). Whole grains can be added when additional carbohydrate energy needs exist beyond what can be achieved with vegetables and fruits. Individuals with early signs of insulin resistance or poor glucose control, vegetables (ideally non-starchy) should be consumed preferentially over fruits, with both taking precedence over whole grains.
Calories from carbohydrates should come in the form of complex carbohydrates, with particular emphasis on vegetables and fruits. The authors of this text recommend that carbohydrate intake be tailored to the activity level of the individual and their weight-related goals.
Water
Water is easily the most important substance consumed daily. People can go months without food, but only a matter of days without water. The human body is composed of ~60% water, on average. Athletes can lose up to 6-10% of body weight as sweat loss, leading to significant dehydration if it is not replenished (Popkin, 2010). Concerningly, performance decrements have been seen at levels of dehydration as low as 2% (Murray, 2007). It is important to ensure that exercisers are appropriately hydrated prior to, during, and after a training session.
How much water should be consumed?
No universal recommendations exist regarding ideal water intake. It varies significantly across people and is highly dependent on activity levels, diet, and how much they sweat. For an average adult man and woman, they probably need around 3.7 liters (122 oz) and 2.7 liters (89 oz) of water, respectively (Popkins, 2010). It is generally impractical to have people track and measure this, however some simple tools exist to determine if a person is consuming enough water.
Thirst is the most obvious indicator that someone is dehydrated but people may not feel thirsty until they are already significantly dehydrated. Probably the easiest and most reliable way to gauge if a person is appropriately hydrated is the color of their urine. In a hydrated state, it should be a faint yellow color or clear. The darker the color, the more dehydrated they are. Having exercisers drink some water prior to a training session and allowing them free access whenever they feel compelled to drink during the session can aid in rehydrating them. Instructing them to monitor their urine color throughout the day to adjust their water intake appropriately can empower them to stay hydrated.
Hydration can be assessed by using the color of the urine, with adequate hydration resulting in a faint yellow or clear urine color.
"Diets”
A diet is simply the food and drink that are habitually consumed. The connotation when someone goes on a “diet” is that they are restricting food in some fashion. The three ways one can diet are to restrict…
- 1.1) what they eat (i.e., avoiding carbohydrates),
- 2.2) how much they eat (i.e., limiting calories), or
- 3.3) when they eat (i.e., intermittent fasting).
All diets operate on at least one, and potentially all three of these principles.
To lose weight, an energy deficit must be created by either decreasing intake (technically, what is absorbed) or increasing the number of calories burned. Eating less can be accomplished by either restricting the type of food being eaten, the amount of food being eaten, or the window in which food is consumed.
Recognizing that the Standard American Diet (appropriately coined the SAD diet) is arguably the least healthy diet one can create, making any deviation or purposeful change from it will lead to better health. This is one of the reasons why there is so much seemingly conflicting nutrition research. Comparing any dietary change to the worst diet available makes it seem like a “healthier” diet.
There are an infinite number of fad diets promising fast weight loss, increased energy, and delicious food but none that will work for everyone. While it is beyond the scope of this text to review and endorse specific diets, understanding the role of diet and exercise with regards health promotion and weight loss is helpful.
Though not a “diet,” arguably the best dietary advice was coined by investigative journalist, Michael Pollan in seven words “eat food, not too much, mostly plants (Pollan, 2006).”
Low-Fat Diets
The low-fat craze of the 1980s and 1990s arguably paved the way for the obesity epidemic. The concept of eating fat causing one to become fat made theoretical sense. Fat has the highest caloric content per gram compared to carbohydrates or protein and is generally less satiating. What ultimately matters though is if the individual consumes more calories than they need. However, this excess can be in the form of fat, carbohydrate, or protein.
The “failure” of the low-fat diet to improve health in the US is somewhat of a misrepresentation. While the percentage of calories Americans consumed coming from fat did decrease during this period, it wasn’t technically a low-fat diet. Most importantly, the absolute number of calories increased overall! A percentage can decrease by consuming less of the food of interest or by increasing the number of other foods relative to that. Americans ate more non-fat calories, leading to weight gain and obesity.
Companies removed the fat out of products to meet consumer demand and instead infused them with sugar and processed carbohydrates. People felt less satiated by these highly processed foods and ended up eating more of them to feel full. Low fat labels misled consumers to thinking that they were “healthy,” even though these were products had little health benefits and led to their increased consumption.
That said, a well-formulated low-fat diet can promote health and longevity. Arguably, some of the healthiest diets on the planet are low in fat (Buettner, 2016). For individuals who are otherwise metabolically healthy, a diet that is lower in fat can provide ample carbohydrate (glycogen) for resistance training sessions, as well as sufficient protein and fat to aid in recovery. Focusing on whole plant foods, lean sources of protein, and healthy sources of fat are sound dietary principles (Lichtenstein, 2006).
Low Carb Diets
Unlike the other two macronutrients (fat and protein), there is no minimal level of carbohydrates necessary to sustain life. This becomes particularly relevant when a person’s goal is to reduce body fat. This requires creating a caloric deficit, and carbohydrates are typically the “easiest” foods to reduce. Decreasing carbohydrates also has the added benefit of lowering the amount of insulin the body uses to store them.
New research has emerged to suggest that low carb diets may be suitable or potentially beneficial for endurance athletes (Chang, 2017), though this does not apply to resistance training. To reap these potential benefits, it requires several months of adaptation. This process results in the body substantially upregulating its ability to oxidize fat. This would theoretically be preferable for endurance events such as marathons and ultra-marathons where the body has insufficient carbohydrate (glycogen) stores to supply energy throughout these events. By preferentially shifting metabolism towards fat utilization, sustained energy could be provided throughout the duration of the event, avoiding the “bonk,” or difficult metabolic transition from carbohydrates to fat that occurs in the later stages of these long-distance sessions. This has not been definitively shown in well done studies, so more research is needed to determine what, if any performance benefits can be achieved from consuming a low carbohydrate diet (Cao, 2021).
For individuals with diabetes and signs of insulin resistance, diets lower in carbohydrates can aid in blood glucose control and insulin resistance (Boden, 2005) (Athinarayanan, 2019). For these individuals, healthy fats, which have no impact on blood glucose or insulin, should be the mainstay of the diet. Additional energy needs can be met with nutrient dense complex carbohydrates consisting primarily of vegetables with some fruits.
Losing “Water Weight”
Losing “Water Weight”Because water makes up such a high proportion of body weight, it can have a marked impact on the “scale weight” that people see. An individual that is incredibly dehydrated could easily be 2-3 pounds “lighter” on the scale, as compared to an individual that is over hydrated, who could gain 1-2 pounds. None of this represents fat loss and will come and go depending on the person’s hydration level. Hydration can also impact body fat measuring devices, particularly the bioelectrical impedance measures, which can read inappropriately high or low depending on the hydration status.Losing “Water Weight”Because water makes up such a high proportion of body weight, it can have a marked impact on the “scale weight” that people see. An individual that is incredibly dehydrated could easily be 2-3 pounds “lighter” on the scale, as compared to an individual that is over hydrated, who could gain 1-2 pounds. None of this represents fat loss and will come and go depending on the person’s hydration level. Hydration can also impact body fat measuring devices, particularly the bioelectrical impedance measures, which can read inappropriately high or low depending on the hydration status.
If people are going to track their weight, it is recommended that they do it at the same time each day, at the same hydration level. This is best accomplished by having them weigh themselves first thing in the morning before they eat or drink anything.
The other important aspect of water regarding body weight, beyond hydration, is that every gram of carbohydrates stored as glycogen holds three grams of water (Fernandez-Elias, 2015). If glycogen is used for energy and not replaced, or if a person is on a low carbohydrate diet, there will be an illusion of scale “weight loss.” This does not represent actual fat loss (which is the goal), and this weight will be “regained” as soon as glycogen stores are repleted. This phenomenon is one of the reasons why low carbohydrate diets yield such rapid “weight loss” when they are first started. Creating caloric deficit is the only way to lose actual body fat.
Understanding Fat Loss and the Role and Type of Exercise
After water (comprising ~60% of body weight) the next largest percentage of body weight is comprised of protein (the largest store of protein is in the form of lean muscle tissue), fat, and carbohydrates (stored glycogen) (Wang, 2011). The remaining bodyweight mass consists of calcium and cartilage (skeleton), skin, hair, organs, secondary soft tissue (ligaments, tendons, etc.), and other minerals.
The body reaches full growth capacity by the mid-20s, therefore the weight of most of the above is set by then. The amount of stored water and glycogen are kept within a small window. This means when we gain and lose weight in adulthood, it is primarily in the form of fat and protein (lean muscle).
While it’s possible to increase protein (lean muscle) stores in adulthood through resistance training and adequate protein intake, for most people the increase in muscle weight will not be a significant percentage of overall bodyweight. This means that for most people, the increase or decrease in bodyweight in adulthood is primarily in the form of fat. To make matters worse, it is important to realize that muscle mass continually decreases during the entire aging process at a rate of 3-8% per decade after the age of 30 and an even higher rate after the age of 60 (English, 2010). However, this rate of decline can be slowed by resistance training and consuming adequate levels of protein (English, 2012) (Lavin, 2019).
As mentioned previously, with few exceptions, fat is only lost while the individual is in a caloric deficit – meaning that their body is burning more calories than it is ingesting. Therefore, creating a caloric deficit is the primary method for fat loss (Strasser, 2007). A caloric deficit can be obtained by:
- 1.Consuming (technically absorbing) fewer calories.
- 2.Increasing energy expenditure.
Combining these two approaches yields the best results. However, since a caloric deficit can be created through diet alone, a person can burn and lose fat without doing any exercise at all. The notion that a certain type of exercise or specific intensity must be performed to oxidize (burn) or lose fat is simply not true.
Views like “You must…
- …train in higher repetition ranges with short rest periods,” or
- …use a metabolic conditioning approach,” or
- …train with heavy weights to failure,” or
- …perform hours of aerobic exercise,”
- or any other view surrounding needing to do a specific type of exercise to lose weight is incorrect.
Fat Burning Zone:
Fat Burning Zone:Fat is the predominant fuel that is burned for energy at rest, and until exercise intensity reaches greater than 65% of VO2 max (Melzer, 2011). The notion of the “Fat Burning Zone” within exercise is nonsensical and should not be perpetuated.The concept correctly recognizes that an individual can burn a higher percentage of fat at lower exercise intensities, however the absolute number of calories will be much less. Fat Burning Zone:Fat is the predominant fuel that is burned for energy at rest, and until exercise intensity reaches greater than 65% of VO2 max (Melzer, 2011). The notion of the “Fat Burning Zone” within exercise is nonsensical and should not be perpetuated.The concept correctly recognizes that an individual can burn a higher percentage of fat at lower exercise intensities, however the absolute number of calories will be much less.
For individuals who want to “burn fat,” they are better suited for exercising at higher intensities that allow for great caloric expenditure, and thus, create a large caloric deficit.
If the person is in a caloric deficit, all exercise approaches will assist in the fat burning or fat loss process, because all exercise approaches increase caloric expenditure.
Having said that, the proportion of fat mass and lean mass that are lost can vary dramatically depending on how the caloric deficit is achieved. Optimizing fat loss and minimizing lean mass loss during a caloric deficit is best achieved by ensuring that there is:
- 1.Adequate protein intake (at least 1.6 g/kg of body weight).
- 2.An appropriate resistance training program, preferably a Flexible Linear Periodization model that utilizes a spectrum of repetition ranges (e.g., 4 to 15) at an intensity of “at or near muscle failure.”
This is how all or most lean muscle tissue is maintained while in a caloric deficit, so that the weight that is lost comes mostly in the form of fat (Yasikolka, 2016).
If an individual is in a caloric deficit and only doing aerobic exercise, using light weights to resistance train, or rarely going to “at or near muscle failure,” fat will still be lost but a much higher proportion of lean mass will go along with it. This is detrimental because skeletal muscle is more metabolically active than fat. Maintaining 1 lb. of skeletal muscle burns ~6 calories per day (or 13 calories/kg), whereas fat mass only burns ~2 calories per day (or 4.5 calories/kg) (Wang Z. Y., 2011). Although this seems like a relatively small number of calories, over time it can make a huge difference in being able to maintain an individual’s weight.
Muscle is more metabolically active than fat, with each pound of muscle burning an extra 4 calories per day as compared to a pound of fat.
From an exerciser’s perspective, although their goal may be weight loss, they are generally interested in looking better. Because lean mass is denser than fat mass, it is possible for a person to “look better” and like they have lost weight, even if their scale weight does not change. A lower percentage of body fat, as opposed to scale weight, is what people are really after.
Overall Dietary Recommendations
Dietary advice for people should be tailored to their individual goals, underlying physiology, and cultural preferences. Understanding the general recommendations throughout this chapter can provide a helpful framework to start.
Dietary protein needs should be met first, fat needs second, and then the remainder of the allotted calories should come in the form of complex carbohydrates, prioritizing vegetables and fruits.
Table 10.7: Daily Macronutrient Recommendations.
Table 10.7: Daily Macronutrient Recommendations.
| Macronutrient | Amount per Day | Percent of Calories |
|---|---|---|
| Protein | ~1.6 g/kg (0.73 g/lb) | ~10-20% |
| Fat | ~1 g/kg (0.45 g/lb) | ~20-35% |
| Carbohydrates | >130 g (Remaining calories after protein and fat needs are met) | ~45-70% |
Table 10.8: Example Macronutrient Composition for a 150 lb. (68 kg) male on a 2,500 calorie diet.
Table 10.8: Example Macronutrient Composition for a 150 lb. (68 kg) male on a 2,500 calorie diet.
| Macronutrients | Percent of Calories |
|---|---|
| Protein: 1.6 g/kg x 68 kg = 109 g x 4 cals/g = 436 cals Fat: 1 g/kg x 68 kg = 68 g x 9 cals/g = 612 calories Carbs: 2500 cals - 436 cals (Protein) - 612 cals (Fat) = *1452 cals | 17% protein ~25% fat 58% carbs |
*Note: 1452 calories is equal to 363 grams of Carbs
Although much of this chapter was spent exploring the various macronutrients and offering target ranges for each, people eat food, not nutrition facts. Understanding the importance of appropriate macronutrient intake is important for fitness professionals but when dealing with clients, it may be more helpful to think about healthy dietary patterns, as opposed to rigid macronutrient prescriptions.
A low carb or low-fat diet can be healthy, but it depends on what foods are being eaten as part of that diet. Pork rinds are low carb and Pixy Stix are fat free. The most recognized and studied healthy eating patterns include the Mediterranean diet (Davis, 2015) (Estruch R. R., 2018), the Dietary Approach to Stop Hypertension (DASH) diet (Appel, 1997), and vegetarian or plant-based diets (Kim, 2018) (Wright, 2017). Other popular diets, such as the paleolithic diet exist, but are far less studied from a research perspective. Absence of evidence is not evidence of absence, meaning that the diet could be healthy, but we don't have the data to assess it, yet. Anecdotally, many people may seem to respond well to some of these “new diets,” but more research is needed to validate these claims. Again, remember that making almost any dietary change from the SAD eating pattern in the US will make people look and feel better. When clients are interested in less studied approaches, it is important to work with their physician or a dietician to ensure that their body is responding well to the approach (see Advance Nutrition Framework section).
Having clients focus on consuming a predominantly whole food, plant-based diet that meets their macronutrient and dietary needs can guide clients toward healthier choices (Katz, 2014) (Micha, 2017). For people who respond well to visuals, the Harvard Healthy Plate provides a convenient image to review with clients on how their meals should look (link: https://www.hsph.harvard.edu/nutritionsource/healthy-eating-plate/).
Advanced Nutrition Framework
The interaction between various foods and our bodies is incredibly complex. There is little contention that what we eat has widespread health implications. A 2018 review article found that poor diet was the number one risk factor for death and disability (Collaborators, 2018). While much of this chapter focused on macronutrient composition and food being the fuel for exercise and substrate for recovery, it is important to appreciate that the optimal diet for overall health and longevity needs to consider more than body weight and performance. Specifically, an optimal diet should address six health areas:
- Energy Balance (i.e., gaining, maintaining, or losing weight as appropriate).
- Lipoproteins (i.e., cholesterol levels).
- Insulin sensitivity and blood glucose levels.
- Inflammation.
- Gut “microbiome”.
- Toxins.
While it is beyond the scope of this text to explore all six areas of health that nutrition effects, recognizing the far-reaching impact of diet and health is important. This complexity highlights the need to partner with a dietician or health care provider to prescribe tailored dietary recommendations to clients. Ensuring a balanced diet becomes more important when a person is eating in a caloric deficit or following a restrictive diet, as this can lead to inadequate intakes or deficiencies of specific nutrients.