Full chapter reading
Chapter 16: Common Neurological Conditions
Introduction
Neurological conditions such as Parkinson’s disease (PD) and multiple sclerosis (MS) pose significant challenges to mobility, strength, and overall quality of life. This chapter explores the essential role of exercise in managing these progressive conditions, emphasizing its ability to improve motor function, reduce symptoms, and enhance physical and emotional well-being.
The first section focuses on Parkinson’s disease, detailing the benefits of resistance training, aerobic exercise, and balance activities in addressing motor symptoms like tremors, rigidity, and bradykinesia. Practical considerations for program design include tailoring exercises to the severity of the condition and collaborating with healthcare teams to ensure safety and efficacy.
The second section examines multiple sclerosis, emphasizing the importance of structured exercise to combat fatigue, improve muscle strength, and manage spasticity. The guidelines address the need for careful monitoring, progressive adaptations, and strategies to mitigate heat sensitivity and other symptoms.
Together, these sections present evidence-based strategies for fitness professionals to create programs that support functional independence, reduce disease progression, and improve quality of life for individuals with PD and MS.
Section 1: Parkinson’s Disease
Parkinson’s disease (PD) is the second most common neurodegenerative disorder after Alzheimer’s disease. It affects approximately six million people worldwide. It is a chronic and progressive neurological disease that affects predominately dopamine-producing neurons in a specific area of the brain called substantia nigra. Studies have shown that individuals with PD display greater motor unit loss and disrupted motor unit recruitment patterns compared with age-matched non-PD controls. Both motor unit loss and disruption of motor unit recruitment are notable signs of motor unit remodeling that might be indicative of heightened incidence of denervation and myofiber grouping compared with age-matched, non-PD controls (Parkinson's Foundation, 2019).
According to the Parkinson’s Foundation, there are five stages which define this condition:
1. Stage one: During this initial stage, the person has mild symptoms that generally do not interfere with daily activities. Tremor and other movement symptoms occur on one side of the body only. Changes in posture, walking and facial expressions occur.
2. Stage two: Symptoms start to worsen. Tremor, rigidity and other movement symptoms affect both sides of the body. Walking problems and poor posture may be apparent. The person is still able to live alone, but daily tasks are more difficult and greater in duration.
3. Stage three: Considered mid-stage, loss of balance and slowness of movements are hallmarks. Falls are more common. The person is still fully independent, but symptoms significantly impair activities such as dressing and eating.
4. Stage four: At this point, symptoms are severe and limiting. It’s possible to stand without assistance, but movement may require a walker. The person needs help with activities of daily living and is unable to live alone.
5. Stage five: This is the most advanced and debilitating stage. Stiffness in the legs may make it impossible to stand or walk. The person requires a wheelchair or is bedridden. Around-the-clock nursing care is required for all activities. The person may experience hallucinations and delusions.
The symptoms of PD develop slowly over years and symptom progression rates vary from person to person. People with PD may experience tremors, both at rest and with action, bradykinesia (slow movement), rigidity of the spine, trunk, and extremities, stooped posture, frequent falls, and issues with gait and balance. Non-motor symptoms may impact people with PD more than motor symptoms. These symptoms include apathy, depression, constipation, sleep behavior disorders, impaired sense of smell and swallowing, cognitive decline, mood disorders, hallucinations, vision problems, impulsive behaviors, and fatigue.
There is no standard treatment for people with PD. The primary interventions to treat PD are medications, brain surgery, and exercise. The medications primarily treat the symptoms, so frequently a patient with PD is on multiple medications throughout the day. No treatments are currently available to reverse the course of this disease.

A growing body of evidence strongly supports exercise as a primary intervention to improve the motor and non-motor symptoms of PD. Individuals with PD benefit from resistance exercise, along with aerobic, flexibility, balance, and gait training (Uhrbrand, 2015). The general exercise guidelines found in this section apply to those with mild to moderate Parkinson’s disease, as they will likely benefit from engaging in a progressive, Flexible Periodization program. It is outside of the scope of this section to make recommendations for more severe cases of this disease, as these individuals would likely need specialized care.
In a fitness professional-client relationship, the fitness professional should make the determination if they have the knowledge and skill to work with this type of client. If they do not feel comfortable or that it’s appropriate, it is always acceptable to refer the patient out to someone with more experience. Assuming the fitness professional feels comfortable with the client, it is advised that the fitness professional connect with the client’s practitioners (e.g., primary care, neurologist, physical or occupational therapist). It is helpful to learn about any necessary restrictions that need to be considered, areas that should be emphasized within program design, and other information that the practitioner deems important.
Based on cognitive ability, the individual should be allowed input and some autonomy with program design. This will help develop trust, place them more at ease, and ensure that the fitness professional-client relationship will function as a true team.
Initial Exercise Assessments
- Flexibility and trigger point assessment. The fitness professional or exerciser should incorporate the flexibility and trigger point assessments as described in Chapter 7 along with the additional considerations described in Chapter 11. If it is difficult for the individual to get up and down from the floor, trigger point assessments may need to be performed with the use of The Stick or a similar tool for the lower body. Tools can also be placed against a wall for the person to lean their upper body into them.
- Cardiovascular assessment. The fitness professional or exerciser can follow the guidelines in Chapter 5 along with the additional considerations in Chapter 11. If the person is not able to perform an assessment on a treadmill, bicycle, or elliptical, the Rockport walking test may be a proper choice. An alternative would be a UBE (upper body ergometer) for those who are not able to sustain aerobic activity with the use of their legs.
- Strength assessment. The fitness professional or exerciser should incorporate the strength assessment as part of the Familiarization Phase, as described in Chapter 6.
Program Design Considerations
- Cardiovascular program design. Individuals with PD should engage in aerobic exercise four to six days per week, 20 to 60 minutes per session (when appropriate), at an RPE of 4 to 6. The goal should be to obtain 150 to 300 minutes of moderate- to vigorous-intensity aerobic exercise each week. Exercisers who are not able to sustain 20 consecutive minutes should be instructed to find their appropriate baseline of duration and intensity (as described in Chapter 5) and progress from there.
For those with mild PD, high-intensity interval training can be implemented within training sessions once the person can maintain 20 minutes or greater of continuous aerobic exercise at an RPE of 4 to 6. If high-intensity exercise is implemented within the program, overall volume and duration should be low (i.e. cycle through the recovery:work period no more than three times and progress from there); the work portion should be relatively short (e.g. 30 to 60 seconds); and the recovery portion should begin at a 3:1 to 5:1 ratio (e.g. 120 seconds of rest for every 30 seconds of work).
See Chapter 5 for more information on cardiovascular assessment and program design.
Table 16.1: Example Cardiovascular Program Design for a Person with Parkinson’s Disease
| Day | Duration(Minutes) | Intensity(RPE-Talk Test Method) |
|---|---|---|
| Monday | *20 to 60 | (3 to 6 RPE) |
| Tuesday | *20 to 60 | 3 to 6 RPE |
| Wednesday | 10 to 15(assuming mild PD) | **modified high-intensity interval training |
| Thursday | *20 to 60 minutes | 3 to 6 RPE |
| Friday | *20 to 60 minutes | 3 to 6 RPE |
- Or as tolerated and functionally able.
- Including a modified high-intensity interval training session is at the fitness professional or exerciser’s discretion. It is based on fitness level, absence of symptoms, well-controlled resting blood pressure, and positive response to exercise. Recovery portion should be at an RPE of 2 to 3 and work portion at an RPE of 6 to 7.
- For example, recovery to work ratio may begin at 5:1 or 6:1, cycling through each ratio 3 to 5 times (e.g., 2.5 minutes at an RPE of 2 to 3 followed by 30 seconds at an RPE of 6 to 7). See RPE-Talk Test method in Chapter 5 for more detail.
- It is the fitness professional’s responsibility to determine frequency, duration, intensity, and progression on a case by case and session by session basis.
- Strength program design. The fitness professional or exerciser can follow the resistance training guidelines covered in Chapters 4 and 6 with the following additional considerations:
- Always ensure “readiness to train” questions are asked prior to every session. Based on the answers to each question, the volume and intensity of the session should be adjusted accordingly.
- If the exerciser begins to develop any of the following symptoms: light-headedness, dizziness, nausea, pale or clammy skin, excessive sweating, headache, chest pain, chest tightness, heart palpitations, unusual fatigue, blurred vision, or feels anything “other than the norm,” terminate the session and seek medical advice.
- Avoid taking working sets to muscle failure.
- Following the low volume, low intensity Familiarization Phase, The RPE Method should be used as the primary guide for intensity. Working sets should be terminated when the RPE reaches a 6 to 8 (on a 1 to 10 scale).
- Avoid exercises that are too complex or challenging.
- Avoid the Valsalva maneuver.
Table 16.2: Example Resistance Training Program Design for a Person with Parkinson’s Disease
| Phase | Length of Phase | Intensity(The RPE Method) |
|---|---|---|
| Familiarization(initial program design) | As needed. Typically, 3 to 4 weeks. | 4 to 6 RPE |
| 15 to 20 repetitions per set | 3 to 4 weeks | 5 to 7 RPE |
| 12 to 15 repetitions per set | 3 to 4 weeks | 5 to 7 RPE |
| 10 to 12 repetitions per set | 3 to 4 weeks | 5 to 8 RPE |
| 8 to 10 repetitions per set | 2 to 3 weeks | 5 to 8 RPE |
- Following the first or second cycle of the above four suggested phases (following the Familiarization Phase) the loading zones may be shifted to 12 to 15 reps/set, 10 to 12 reps/set, 8 to 10 reps/set, and 6 to 8 reps/set at the discretion of the fitness professional, the exerciser, and their healthcare provider (if appropriate). This should be based on fitness level, absence of symptoms, well-controlled resting blood pressure, and positive response and natural progression to exercise.
- It is the fitness professional or exerciser’s responsibility to determine repetition ranges, phase lengths, and session intensities on a case by case, session by session basis.
Table 16.3: General Scope of a Week
| Guidance |
|---|
| Vary Intensities from low to moderately high using The RPE Method |
Table 16.4: Flow and Intensity of an Individual Resistance Training Session
| Exercise | Intensity |
|---|---|
| Readiness to train | Always begin with Readiness to Train questions and adjust or terminate sessions appropriately and accordingly |
| Trigger Point Release | Low |
| Dynamic Warm-up | Low to Moderate |
| Core Warm-up | Low to Moderate |
| Total Body Workout | Use The RPE Method |
Additional Considerations
- Emphasize hydration before, during, and after sessions.
- All exercise should start 45 to 60 minutes after the individual has taken any medication(s).
- Always monitor for worsening Parkinson’s symptoms (e.g., increases in dystonia, the slowing of movement, tremors, freezing). If identified, their medical team should be notified.
- Initially rest periods between resistance training sets should be long enough to allow heart and breathing rate to return to at, or near, resting.
- If the person has the cognitive and functional ability to perform static (e.g., single leg standing) and dynamic (e.g., backwards walk, side shuffle, and step-downs) balance, these types of exercises should be included within the program design.
- If they suffer from joint pain, follow the guidelines suggested in Chapter 12 for knee, low back, hip, and neck “friendly” exercises.
- Aerobic exercise program design should begin with low intensity and the duration should be based on mental and physical tolerance.
The Case for Progressive Resistance Training as a Primary Intervention
When designing exercise programs for individuals with Parkinson's disease (PD), the primary goals should extend beyond merely maintaining current levels of functionality. Instead, the focus must be on improving conditioning, strength, power, and lean muscle tissue – common theme throughout this book. These adaptations not only enhance overall fitness but also contribute significantly to fall prevention, improved activities of daily living (ADLs), and a better quality of life. However, most popular programs offered for individuals with PD fail to adequately target these critical adaptations.
Popular Programs and Their Limitations Programs such as yoga and Rock Steady Boxing have gained popularity due to their accessibility and engagement. While these modalities provide some benefits—yoga improves flexibility and balance, and boxing enhances conditioning and coordination—they lack the progressive stimuli required to achieve meaningful increases in strength, power, and lean muscle. Even yoga, which can build some strength and balance, is inherently limited in its ability to progress individuals beyond beginner-level strength compared to established norms.
Rock Steady Boxing, while excellent for cardiovascular conditioning and motor coordination, focuses almost exclusively on these domains, with minimal emphasis on the progressive resistance needed to improve muscle strength or power. These limitations highlight the need for these programs to serve as supplements to a progressive, periodized resistance training program, rather than as standalone interventions.
The Importance of Progressive Resistance Training As discussed in earlier chapters, the principles of progression, overload, and accommodation are non-negotiable when aiming to elicit meaningful physiological adaptations. Resistance training (RT), when designed to include progressive overload, ensures that the neuromuscular system is consistently challenged, driving improvements in maximal strength, power, and muscle hypertrophy. These adaptations directly address the deficits seen in individuals with PD, such as reduced force-generating capacity and impaired functional performance.
Research supports this approach, as highlighted in the study by Helgerud et al. (2020). The authors emphasize that traditional rehabilitation programs often underdose intensity, leading to limited neuromuscular and functional gains. Their findings demonstrated that maximal strength training (MST), performed at ~90% of one repetition maximum (1RM) with an emphasis on lifting loads with maximal concentric velocity, significantly improved not only strength and power but also functional tasks such as stair climbing and the Timed Up and Go (TUG) test.
While the specific MST protocols used in the study may not translate directly into general programming for individuals with PD, the key takeaway is clear: strength training programs for this population must prioritize intensity and progressive overload. Without these elements, individuals are unlikely to experience the neuromuscular and functional improvements necessary for meaningful gains in independence and quality of life.
Application of Principles in PD-Specific Training To achieve the desired outcomes, resistance training for individuals with PD should adhere to the following principles:
- Progression: Gradually increase the load, volume, or intensity to challenge the neuromuscular system.
- Overload: Ensure that training intensity is sufficient to stimulate adaptation, typically within the 6-12 repetition range for strength and power improvements.
- Periodization: Implement flexible, linear periodization to optimize adaptation and recovery, cycling through phases that target strength, endurance, and power.
Reinforcing the Value of Comprehensive Programming While supplemental programs such as yoga and boxing can enhance engagement and address specific aspects of physical fitness, they must not replace a structured, progressive resistance training program. Only through targeted RT can individuals with PD build the strength, power, and muscle tissue necessary to prevent falls, improve ADLs, and combat the neuromuscular decline associated with the disease. As fitness professionals and healthcare providers, it is imperative to prioritize these principles to ensure optimal outcomes for this population.
Section 2: Multiple Sclerosis
Introduction
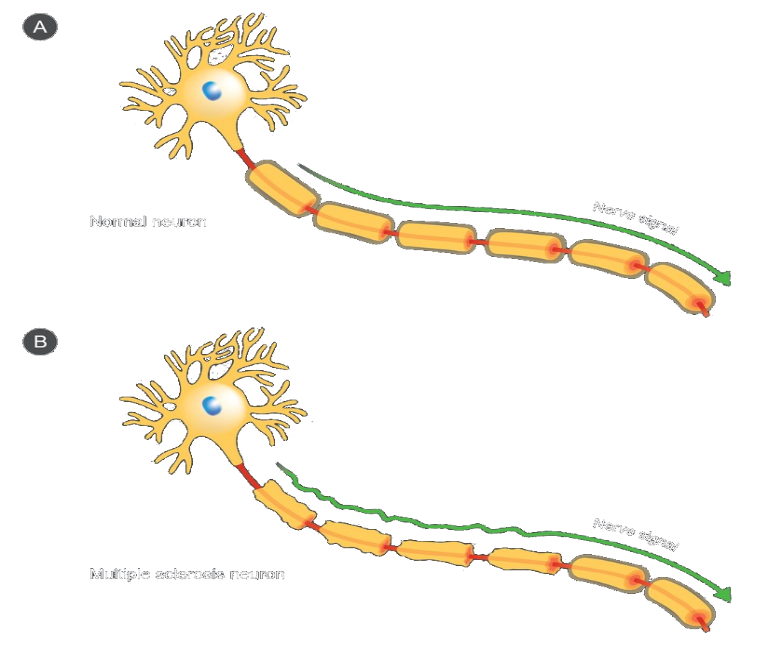
Multiple sclerosis (MS) is typically a relapsing and progressive degenerative neurological disease that affects over two million people worldwide. Most people with MS are diagnosed between the ages of 20 and 50, and it affects two to three times more women than men (National Multiple Sclerosis Society, 2019). The cause of MS is currently unknown. Similar to PD and other neurological conditions, the symptoms and severity vary widely among individuals. Some people with MS look, function, and feel completely “normal,” while others may have episodes with debilitating symptoms. This vast range of symptomatology underscores the need for individual autonomy and the need to focus on the “Flexible” (i.e., basing volume, intensity, and exercise selection on how the individual feels from session to session) aspect of exercise program design.
There are four primary stages of MS:
- Clinically isolated MS: the first episode of neurologic symptoms caused by inflammation and demyelination in the central nervous system.
- Relapsing-remitting MS: this is the most common disease course and is characterized by clearly defined attacks of new or increasing neurologic symptoms. These attacks – called relapses or exacerbations – are followed by periods of partial or complete recovery (remissions). During remissions, all symptoms may disappear, or some symptoms may continue and become permanent. However, there is no apparent progression of the disease during the periods of remission. In other words, the attacks come and go, but the disease doesn’t get worse.
- Secondary progressive: follows an initial relapsing-remitting course. Many people who are diagnosed with relapsing-remitting will eventually transition to a secondary progressive course in which there is a progressive worsening of neurologic function (accumulation of disability) over time.
- Primary progressive: this is characterized by worsening neurologic function (accumulation of disability) from the onset of symptoms, without early relapses or remissions.
Like many diseases, MS is associated with chronic, low grade, systemic inflammation. Many times, individuals who suffer from MS are overweight or living with obesity, inactive (i.e., not meeting minimum exercise guidelines), and have unhealthy eating habits such as diets that are high in processed and sugary foods. Despite the general view that it is a slowly worsening disease over time, there are a growing number of case studies demonstrating that lifestyle medicine (i.e., consuming a healthy diet, exercising, getting adequate sleep, managing stress, and not abusing harmful substances) can help manage, control, and potentially reverse the course and symptoms of this disease. In fact, the author of this text has an intimate personal experience with this disease and a related case study that may help the reader understand what this disease can look like.
My wife was diagnosed with MS in 2004 on her 28th birthday. For the first 5.5 years following the initial diagnosis her health was spiraling downhill. She had daily flare-ups that included migraine headaches, flu-like symptoms, joint pain throughout her body, the “MS hug” (also known as banding or girdling), having her leg lock up or go numb, restless leg syndrome, insomnia, extreme fatigue, nausea, vomiting, and dry heaves.
After beginning a new job, one of her co-workers who suffered from MS offered her some nutrition advice. Willing to try anything, my wife cleaned up her diet. At the same time, I was learning more about the disease from an exercise program design standpoint and placed her on a Flexible Periodized resistance training and RPE-based aerobic exercise program. This combination eventually led to a decrease in her symptoms and less need for using medications. What followed was an amazing reversal of symptoms and disease course. Her strength and overall fitness continued to improve, to the point where her flare-ups significantly decreased in frequency, duration, and magnitude.

She moved from daily flare-ups which were many times debilitating and painful to no major flare-ups in over 5 years! Now in her late-40s, she is stronger, healthier, and more fit than most people who have never been diagnosed with a disease.
A great account of her amazing success story can be found here: https://www.youtube.com/watch?v=u18iRPSN9_A&t=8s
While the situation will be different for everyone, the purpose for describing the above case study is to make the following important points, which apply not only to individuals who suffer from multiple sclerosis, but for those who suffer from any condition:
- Being diagnosed with disease doesn’t need to be or feel like a death sentence.
- Disease management, control, and possible reversal should start with acquiring knowledge about the disease, establishing a positive mindset, and committing to making the changes necessary to improve health, well-being, and quality of life. The fitness professional can play a major role in providing motivation and continued guidance to the client.
- Ensuring that adequate hydration throughout the day and during exercise is critical. This helps regulate the body’s thermostat, reduces the risk of overheating, and can mitigate exacerbations of MS and a variety of conditions.
- If the person has overweight or obesity, emphasis should be placed on slowly reducing bodyfat through diet and exercise (both aerobic and resistance training) over time.
- Focus on improving all aspects of lifestyle medicine. Gradually improving both strength and aerobic capacity, combined with adequate sleep, stress management, and a healthy diet, can reduce chronic, low grade, systemic inflammation. Doing these things alone can prevent, treat, and potentially reverse some cases of MS, as well as prevent up to 80% of the chronic disease that exists (Kjølhede, 2012).
Always keep in mind: A strong and conditioned body is better able to fight disease compared to a weak and deconditioned body.
Working with individuals who suffer from neurological diseases underscores the critical role of Henneman’s Size Principle, discussed in Chapter 1, and its application to progressive resistance training. By systematically reducing repetition ranges (e.g., transitioning from an 8-repetition phase to a 6-repetition phase) while incrementally increasing the load, exercisers can maximize motor unit recruitment, a process fundamental to improving neuromuscular function. Achieving this requires training at an intensity where movement velocity visibly slows, corresponding to a rate of perceived exertion (RPE) of 7 or higher on a 1-10 scale. At this level of effort, heavier loads and lower repetition ranges recruit a greater number and diversity of motor units, activating the full spectrum of the neuromuscular system.
Progressive resistance training not only strengthens muscles but also enhances the neural "electrical grid"—the intricate communication network between the central nervous system (CNS) and muscles. This improved neural drive can promote the creation of new signaling pathways and support neural plasticity, the nervous system's ability to adapt and reorganize itself.
Over time, these adaptations can facilitate recovery and even healing in those with neurological conditions by enhancing motor neuron firing rates, synchronization, and coordination while increasing inter- and intramuscular communication.
In this context, the axiom “what trains together, gains together” rings especially true. Resistance training’s ability to simultaneously stimulate the muscular and nervous systems positions it as a cornerstone intervention for improving functional capacity and reversing or mitigating the symptoms of neurological diseases like multiple sclerosis.
For people who suffer from neurological disease this is critical to understand.
The combination of progressive resistance training (with controlled and explosive tempos), proper form (i.e., neuromuscular control), proper cueing (providing both internal and external feedback), increasing aerobic capacity, and improving overall conditioning play major roles in creating neuroplasticity. These should all be emphasized as first-line interventions in neurodegenerative disease management.
Additional Considerations
- Emphasize hydration before, during, and after sessions.
- Initially rest periods between resistance training sets should be long enough to allow heart and breathing rate to return to at, or near, resting. This reduces the risk of overheating.
- Exercise in a cool environment whenever possible; avoid exercising in hot and humid environments.
- Include exercises which challenge static (e.g., single leg standing) and dynamic (e.g., backwards walk and step-downs) balance.
- If the exerciser is able, progression should include multi-directional lunges within the resistance training program.
- If the individual suffers from joint pain, follow the guidelines suggested in Chapter 12 for knee, low back, hip, and neck “friendly” exercises.
- Aerobic exercise program design should begin with low intensity. The individual should determine duration based on mental and physical tolerance.
Initial Exercise Assessments
- Flexibility and trigger point assessment. The fitness professional or exerciser should incorporate the flexibility and trigger point assessments as described in Chapter 7 along with the additional considerations described in Chapter 11.
- Cardiovascular assessment. The fitness professional or exerciser can follow the guidelines in Chapter 5 along with the additional considerations in Chapter 11.
- Strength assessment. The fitness professional or exerciser should incorporate the strength assessment as part of the Familiarization Phase, as described in Chapter 6.
Program Design Considerations
- Cardiovascular program design. Individuals with MS should engage in aerobic exercise four to six days per week, 20 to 60 minutes per session (when appropriate), at an RPE of 4 to 6. The goal should be to obtain 150 to 300 minutes of moderate- to vigorous-intensity aerobic exercise each week. Those who are not able to sustain 20 consecutive minutes should find their appropriate baseline of duration and intensity (as described in Chapter 5) and progress from there.
For individuals with mild MS, high-intensity interval training can be implemented within training sessions once they can maintain 20 minutes or greater of continuous aerobic exercise at an RPE of 4 to 6. If high-intensity exercise is implemented within the program, overall volume and duration should be low (i.e., cycle through the recovery:work period no more than three times and progress from there); the work portion should be relatively short (e.g., 30 to 60 seconds); and the recovery portion should begin at a 3:1 to 5:1 ratio (e.g., 120 seconds of recovery for every 30 seconds of work).
See Chapter 5 for more information on cardiovascular assessment and program design.
Table 16.5: Example Cardiovascular Program Design for a Person with Multiple Sclerosis
| Day | Duration(minutes) | Intensity(RPE-Talk Test Method) |
|---|---|---|
| Monday | *20 to 60 | 3 to 6 RPE |
| Tuesday | *20 to 60 | 3 to 6 RPE |
| Wednesday | 10 to 15(assuming mild MS) | **modified high-intensity interval training |
| Thursday | *20 to 60 | 3 to 6 RPE |
| Friday | *20 to 60 | 3 to 6 RPE |
- Or as tolerated and functionally able.
- Including a modified high-intensity interval training session is at the fitness professional or exerciser’s mutual discretion. It is based on fitness level, absence of symptoms, well-controlled resting blood pressure, and positive response to exercise. Recovery portion should be at an RPE of 2 to 3 and work portion at an RPE of 6 to 7.
- For example, recovery to work ratio may begin at 5:1 or 6:1, cycling through each ratio 3 to 5 times (e.g., 2.5 minutes at an RPE of 2 to 3 followed by 30 seconds at an RPE of 6 to 7). See RPE-Talk Test method in Chapter 5 for more detail.
- It is the fitness professional or exerciser’s responsibility to determine frequency, duration, intensity, and progression on a case by case and session by session basis.
- Strength program design. The fitness professional or exerciser can follow the resistance training guidelines covered in Chapters 4 and 6 with the following additional considerations:
- Always ensure “readiness to train” questions are asked prior to every session. Based on the answers to each question, the volume and intensity of the session should be adjusted accordingly.
- If the exerciser begins to develop any of the following symptoms: light-headedness, dizziness, nausea, pale or clammy skin, excessive sweating, headache, chest pain, chest tightness, heart palpitations, unusual fatigue, blurred vision, or feels anything “other than the norm,” terminate the session and seek medical advice.
- Avoid taking working sets to muscle failure.
- Following the low volume, low intensity Familiarization Phase, The RPE Method should be used as the primary guide for intensity. Working sets should be terminated when the RPE reaches a 6 to 8 (on a 1 to 10 scale).
- Avoid exercises that are too complex or challenging. For example, a lunge may be inappropriate, at least initially.
- Avoid the Valsalva maneuver.
Table 16.6: Example Resistance Training Program Design for a Person with Multiple Sclerosis
| Phase | Length of Phase | Intensity |
|---|---|---|
| Familiarization(initial program design) | As needed. Typically, 3 to 4 weeks. | 4 to 6 RPE |
| 15 to 20 repetitions per set | 3 to 4 weeks | 5 to 7 RPE |
| 12 to 15 repetitions per set | 3 to 4 weeks | 5 to 7 RPE |
| 10 to 12 repetitions per set | 3 to 4 weeks | 5 to 8 RPE |
| 8 to 10 repetitions per set | 2 to 3 weeks | 5 to 8 RPE |
- Following the first or second cycle of the above four suggested phases (following the Familiarization Phase) the loading zones may be shifted to 12 to 15 reps/set, 10 to 12 reps/set, 8 to 10 reps/set, and 6 to 8 reps/set at the discretion of the fitness professional, the exerciser, and their healthcare provider (if appropriate). This should be based on fitness level, absence of symptoms, well-controlled resting blood pressure, and positive response and natural progression to exercise.
- It is the fitness professional or exerciser’s responsibility to determine repetition ranges, phase lengths, and session intensities on a case by case, session by session basis.
Table 16.7: General Scope of a Week
| Guidance |
|---|
| Vary Intensities from low to moderately high using The RPE Method |
Table 16.8: Flow and Intensity of a Resistance Training Session
| Exercise | Intensity |
|---|---|
| Readiness to train | Always begin with Readiness to Train questions and adjust or terminate sessions appropriately and accordingly |
| Trigger Point Release | Low |
| Dynamic Warm-up | Low to Moderate |
| Core Warm-up | Low to Moderate |
| Total Body Workout | Use The RPE Method |
Like other conditions, the fitness professional should make the determination if they have the knowledge and skill to train this type of client. If they do not feel comfortable or that it is appropriate, it is always acceptable to refer the patient to someone with more experience. Assuming the fitness professional feels comfortable with the client, it is advised that they connect with the client’s practitioners (e.g., primary care, neurologist, physical or occupational therapist). It is helpful to learn about any necessary restrictions that need to be considered, areas that should be emphasized within program design, and other information that the practitioner deems important.
Fitness professionals should also learn from the client regarding how their condition manifests itself during exercise. This is typically unique to that individual and will vary based on what type of MS they have and the severity of the disease.
The client should be allowed input and some autonomy with program design. This will help develop trust, place them more at ease, and ensure that the fitness professional-client relationship will function as a true team. Since the client lives with and is extremely familiar with their condition, many times the fitness professional can learn from the client. The client input can also help the fitness professional design the optimal program for that individual.
Summary and Practical Application
Summary Chapter 16 highlights the importance of structured, progressive resistance training combined with aerobic exercise as primary interventions for managing Parkinson's disease (PD) and multiple sclerosis (MS). Both conditions benefit from flexible periodization strategies tailored to individual needs, emphasizing gradual progression, proper intensity, and neuromuscular control. By leveraging principles such as Henneman’s Size Principle and progressive overload, these programs stimulate motor unit recruitment, neural plasticity, and overall functional improvement. In addition, lifestyle medicine—including proper hydration, stress management, and balanced nutrition—plays a pivotal role in reducing systemic inflammation and improving outcomes.
The examples and case studies presented underscore the transformative potential of personalized exercise programs for mitigating symptoms, enhancing quality of life, and even reversing disease progression in some cases. Integrating high-intensity interval training (when appropriate) and balance-focused exercises further supports neuromuscular coordination, independence, and safety in individuals with these conditions.
Practical Application For fitness professionals, the practical application lies in designing individualized programs that address the unique challenges and capacities of each client. Here are some key steps for implementation:
- Comprehensive Assessments: Begin with flexibility, cardiovascular, and strength assessments to establish baselines. Incorporate "Readiness to Train" questions to adjust sessions dynamically based on the client’s current condition and symptoms.
- Tailored Resistance Training: Use flexible linear periodization to guide progression, starting with familiarization phases and gradually increasing intensity and complexity. Prioritize exercises that enhance strength, power, and motor unit recruitment without inducing fatigue or exacerbating symptoms.
- Incorporate Aerobic Exercise: Prescribe moderate-to-vigorous aerobic activity (150-300 minutes per week), progressing as tolerated. Include modified high-intensity interval training for those with sufficient fitness levels and absence of contraindications.
- Neuromuscular Engagement: Focus on exercises that challenge balance, coordination, and functional mobility (e.g., static and dynamic balance drills, multidirectional lunges). These exercises support motor unit synchronization and neuroplasticity.
- Lifestyle Integration: Educate clients on the role of lifestyle medicine—hydration, proper nutrition, stress management, and sleep—in enhancing recovery and reducing inflammation. Provide actionable steps for gradual, sustainable improvements.
- Collaboration and Autonomy: Engage with the client’s healthcare providers to ensure safety and alignment. Allow clients to provide input on program design to foster trust and collaboration.
Through these interventions, fitness professionals can help individuals with PD or MS achieve greater independence, improve physical and cognitive functioning, and experience a better quality of life.